

Bleeding is a biological marvel that we all rarely think about. We accidentally cut a finger, apply pressure or sometimes a bandage and move on with our lives unbothered about it. But for people with hemophilia, an injury leading to bleeding is never that simple- this inherited bleeding disorder quietly shapes everyday life in ways many people can never imagine.
Understanding Hemophilia
What is Hemophilia?
Hemophilia is a rare inherited clotting disorder wherein the proteins responsible for clot formation (clotting factors) are deficient thereby causing prolonged bleeding. Hemophilia, which literally means love (philia) of blood (hemo), could lead to profuse bleeding even after a minor injury that may take a long time to stop on its own unless medically intervened.
Video: https://www.youtube.com/watch?v=BoXBuJSURTI
Genetics behind Hemophilia: How is it Inherited
Hemophilia is inherited in an X-linked recessive manner. Females inherit two X chromosomes, one from their mother and one from their father (XX). Males inherit an X chromosome from their mother and a Y chromosome from their father (XY). Since the hemophilic trait is associated with the X chromosome, if a son inherits an X chromosome carrying the trait from his mother, he will have hemophilia. On the other hand, a female must inherit both the X chromosomes carrying hemophilia to be diagnosed with the same.
The Clotting Cascade: A Biological Domino Effect
Before diving further into the vast topic of hemophilia, let us first understand the reason behind hemophilia affecting clot formation. When a blood vessel is injured, a series of proteins in the blood called clotting factors are activated one after another. Each of the 13 factors work in a synchronized manner to contain the bleed by activating one another in a systematic manner. The end result of this cascade is the formation of a strong, stable fibrin clot that seals the injury.
In hemophilia, one of these clotting factors is missing or defective. Without it, the chain reaction breaks down, and a strong clot cannot be formed. This leads to the prolonged bleeding characteristic of the disorder. The specific “domino” that is missing is what determines the type of hemophilia a person has.
Video: https://www.youtube.com/watch?v=vAyrif99sLE
Types of Hemophilia
There are several types of hemophilia, though the two most common are type A and type B. Hemophilia. Type C and acquired hemophilia are rare.
Hemophilia A: Also referred to as classic hemophilia or factor VIII deficiency is one of the most commonest forms of hemophilia accounting for approximately four out of every five cases.
Hemophilia B: It is the second most common type of hemophilia caused by a deficiency of blood clotting factor IX. This is also called Christmas disease or factor IX deficiency.
Hemophilia C: It is a rarer form caused due to deficiency of factor XI. Unlike the other two main types, Hemophilia C is an autosomal disorder thereby affecting both males and females in the same ratio.
Prevalence of Hemophilia
India is estimated to have a total of 1–1.5 lakh hemophilia cases (based on a prevalence of 1 in 10,000 in its 1.4 billion population) but only a total of about 30,000 cases are diagnosed thereby indicating a major healthcare gap among the 80% of undiagnosed cases. Low awareness among the public and healthcare professionals, especially regarding mild cases, leads to missed diagnoses putting such individuals at risk. Moreover, limited access to healthcare facilities in rural areas further complicates the matter. This is suggestive of high vulnerability among undiagnosed and unaware patients.
The Warning signs of Hemophilia
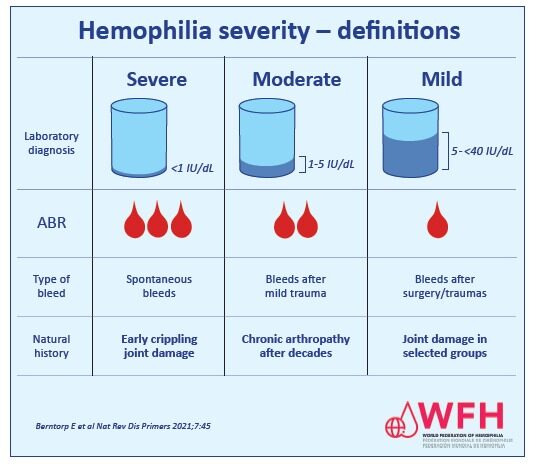
The hallmark of hemophilia is excessive or unusual bleeding. But, the degree of bleeding is dependent on the severity of the condition. Some common symptoms according to the severity of the disease include:
- Mild Hemophilia: People with mild hemophilia A generally experience bleeding typically only after serious injury, trauma, dental procedure or a surgery. Women with mild hemophilia often experience heavy menstrual bleeding, and can hemorrhage (bleed extensively) after childbirth. Usually, people with this condition may remain undiagnosed till adulthood.
- Moderate Hemophilia: People usually suffer from bleeding even after minor injuries.
- Severe Hemophilia: In cases of severe hemophilia, patients often present with internal bleeding, potentially impacting multiple organs. Joints can become painful, swollen, inflamed, and warm and have a restricted range of motion due to bleeding. The most commonly affected joints are the knees, elbows, ankles, shoulders, wrists, and hips. Males are usually diagnosed during circumcision.
The other signs to look out for in Hemophilic patients include:
- Excessive bleeding after routine vaccinations
- Joint pain, swelling, or a feeling of tightness (often caused by internal bleeding)
- Blood in urine or stool (malena)
- Recurrent nosebleeds without a clear trigger (epistaxis)
- In infants, persistent unexplained irritability (which may indicate internal bleeding)
HEMOPHILIA IN FEMALES
HEMOPHILIA CARRIERS
Hemophilia A and B predominantly attract clinical attention in males due to X‐linked inheritance, introducing a bias toward female carriers to be asymptomatic. This common misconception is contradicted by an increasing body of evidence with consistent reporting on an increased bleeding tendency in hemophilia carriers, including those with normal factor VIII/IX levels.
Research suggests that 20–30% of carriers have low clotting factor levels causing bleeding symptoms, such as easy bruising, heavy periods, or bleeding after procedures.
Video: https://youtu.be/DtrtAHLvCJA?si=5EXOtNIBMm5CRt8f
HEMOPHILIA MANAGEMENT IN PREGNANCY
During pregnancy, it is common for your factor VIII levels to rise significantly which can mask up your hemophilia A symptoms. Women who carry the hemophilia A or B mutation or are carriers are at a much greater risk for heavy bleeding after delivery or surgery, such as cesarean section. But, to avoid any unnecessary complications during delivery, it is advised to get your clotting factors checked at least twice during the course of your pregnancy i.e. during the first trimester and late third trimester (32- 34 weeks).
Your anesthesiologist may also not recommend an epidural for labor pain management because of the chance of bleeding around the injection site. Hence, be prepared for different pain management options. The level of your clotting factors will help your healthcare professional determine if an epidural is safe for you.
It is likely that a hemophilic woman, post-delivery may have bleeding from the birth canal that lasts a long time. This is called postpartum hemorrhage and is a medical emergency which needs immediate attention. This can be prevented with prior information.
UNVEILING THE CLOTTING DEFECT: DIAGNOSIS OF HEMOPHILIA
WHO ALL SHOULD GO FOR HEMOPHILIA TESTING
Severe cases of hemophilia are usually diagnosed within the first year of life whereas mild forms might not be apparent until adulthood. Some people learn they are hemophilic only after they bleed excessively during a surgical or dental procedure.
A health care professional might suspect the possibility of hemophilia if:
- There is a family history of Hemophilia – Genetic predisposition
- A newborn has prolonged bleeding from heel prick blood test or following circumcision
- A child has prolonged bleeding from the mouth after losing a tooth
- A child has unexplained bruising when beginning to crawl or walk
- Prolonged bleeding after injury or surgery
DIAGNOSTIC METHODOLOGIES
Hemophilia is diagnosed firstly by doing some screening tests followed by clotting factor tests to confirm the results.
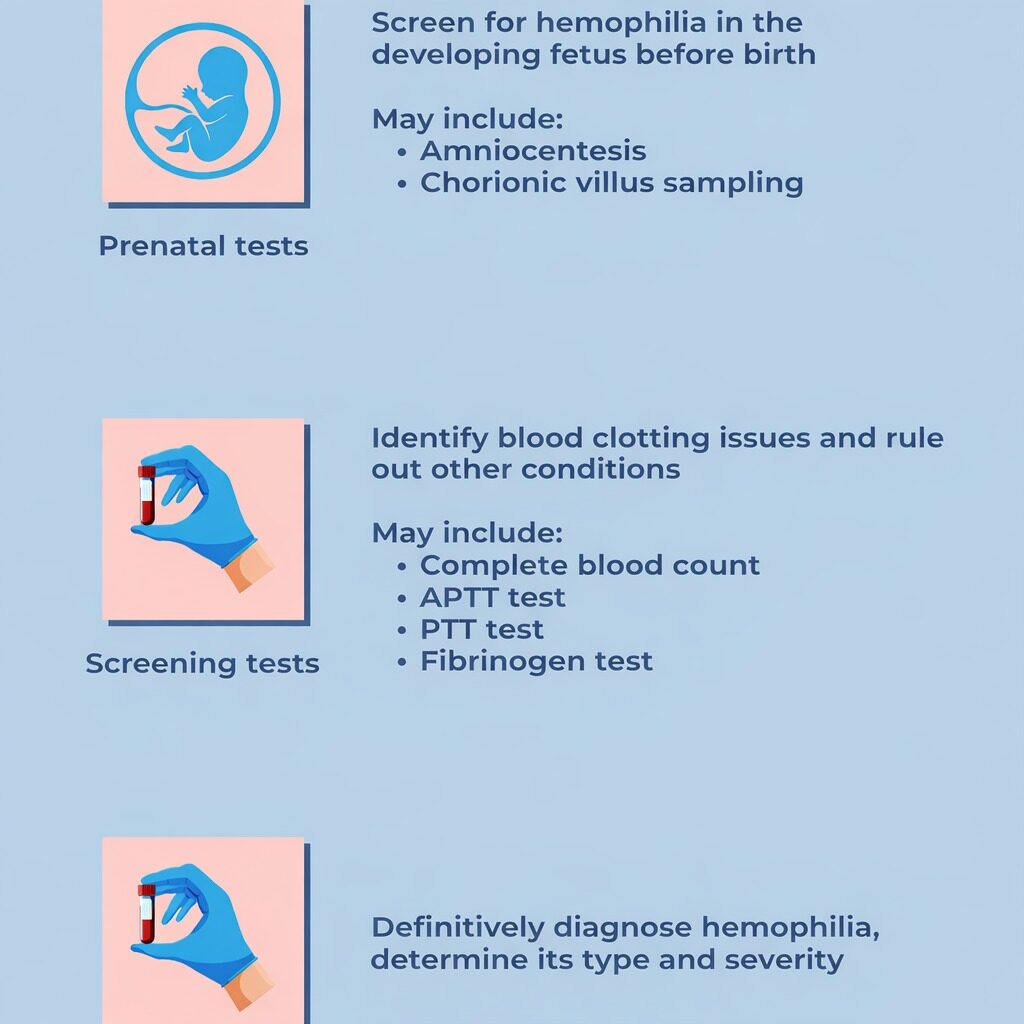
SCREENING TESTS
Screening tests are done to assess the time required for clot formation and to also assess if the blood is clotting properly or not.
The main tests done during screening include:
Complete Blood Count (CBC): It provides a quantitative idea of the amount of hemoglobin (the red pigment inside red blood cells that carries oxygen), WBC count, RBC count and platelets found in the blood. Although the CBC could be normal in hemophilic patients, prolonged bleeding could be reflected as decreased hemoglobin levels in the blood.
Activated partial thromboplastin time (APTT) test: This test assesses the time required for your blood to clot by measuring the clotting ability of factors VIII, IX, XI and XII. Deficiency of particularly factor VIII and IX is characteristic of hemophilia.
Prothrombin time (PT) test: This test also measures the time it takes for blood to clot. It measures primarily the clotting ability of factors I, II, V, VII and X. It is usually normal in hemophilia.
Fibrinogen test: This test is ordered either along with other blood clotting tests or when a patient has an abnormal PT or APTT test result, or both.
CLOTTING FACTOR TESTS
Clotting factor tests are done to confirm the above findings as well as diagnose the type and severity of hemophilia. These tests help to determine the clotting activity of factors VIII and IX in the blood which are the primary proteins responsible for clot formation. Knowing the severity of this bleeding disorder helps in deciding the plan of treatment for the patient.
PRENATAL DIAGNOSIS
Prenatal diagnosis in hemophilia involves specialized tests offered to families at risk of passing on the condition. These tests can confirm early in pregnancy whether their child (developing fetus) may or may not be affected, allowing parents to make informed decisions about whether or not to continue the pregnancy. The results can also help healthcare professionals plan the safest method and location for delivery. Discussing prenatal diagnosis before becoming pregnant is recommended, so individuals fully understand their options. This early discussion supports informed family planning and preparedness.
DELETERIOUS EFFECTS OF LATE DIAGNOSIS
A lack of a family history is an impediment to achieving a timely diagnosis in severe hemophilia A and is associated with poorer treatment outcomes. Delay between the onset of symptoms and the correct diagnosis of the condition could be lethal in severe cases.
One of the major complications of undiagnosed patients with severe forms of hemophilia is bleeding into the joints – especially the knee joint (hemophilic arthropathy), life threatening bleeds in the brain (intracranial hemorrhage) and nerve damage.
TREATMENT AND MANAGEMENT
TREATMENT
Most patients with mild to moderate form of hemophilia prefer on demand therapy i.e. they take medications only to control acute bleed. Although this method is successful in dealing with acute bleeding episodes, this reactive approach fails to prevent the long-term consequences of repeated fatal bleeding, hemorrhages particularly irreversible joint damage. By the time people go for treatment, irreversible damage might already have taken place. This approach can only afford to give an immediate solution but fails to prevent long term complications of untreated hemophilia.
The most effective strategy for managing hemophilia is prophylactic treatment which essentially means regular infusions of clotting factors VIII or XI to prevent bleeding before it starts. The fundamental goal is to have a constantly sufficient level of clotting factor in the blood, thus avoiding bleeds from occurring in the first place. This is especially important for safeguarding joints against hemarthrosis.
Video: https://www.youtube.com/watch?v=FKwqW9KXvuc
MANAGEMENT
Video: Hemophilia 101: for Emergency and Acute Care Physicians
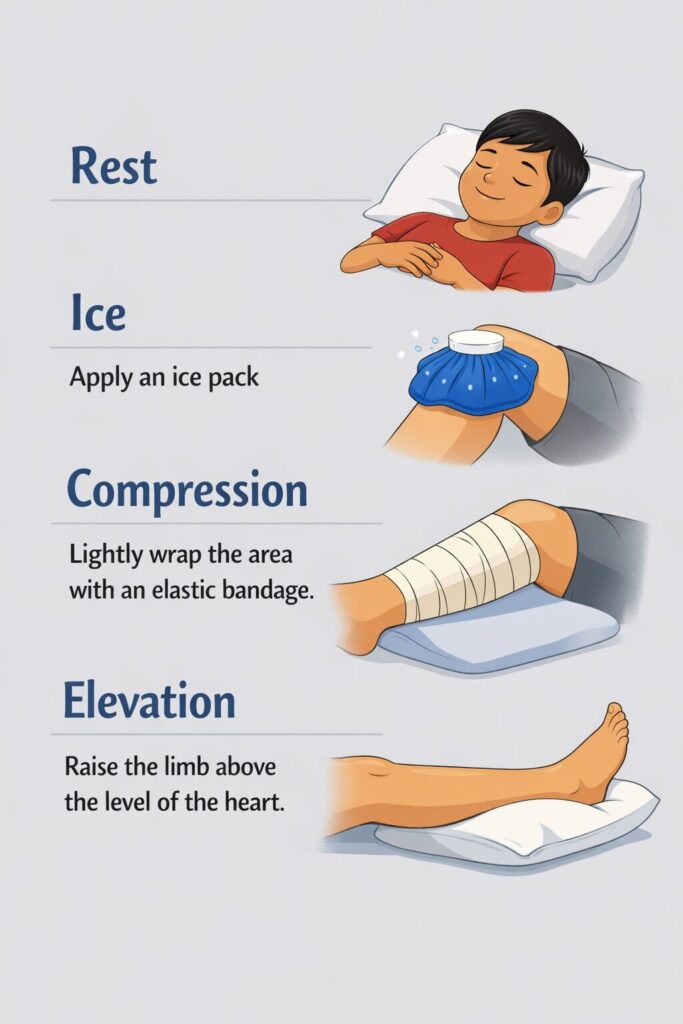
Managing bleeds especially in hemophilia is a daunting task especially if it bleeds into the joint space. The simplest method to control such bleeds is to follow the R.I.C.E method which essentially serves as your first line of defense for immediate first aid.
It is necessary to get your factors replaced as soon as possible at your nearest hospital after a bleeding episode to avoid Internal bleeds.
THE HEMOPHILIA TREATMENT CENTRE: YOUR CARE TEAM FOR EVERY STEP OF THE JOURNEY
A Hemophilia Treatment Center (HTC) is not merely a clinic but a full-time support system. You’ll see experts like hematologists, nurses, a physiotherapist, and a social worker who are all required to help you navigate through your hemophilia journey. They guide your treatment and teach you self-administration factor injections. People treated at HTCs often have fewer complications and better health thereby it is one of the most trusted places for people suffering from bleeding disorders.
TRAVELLING GUIDELINES FOR HEMOPHILIACS
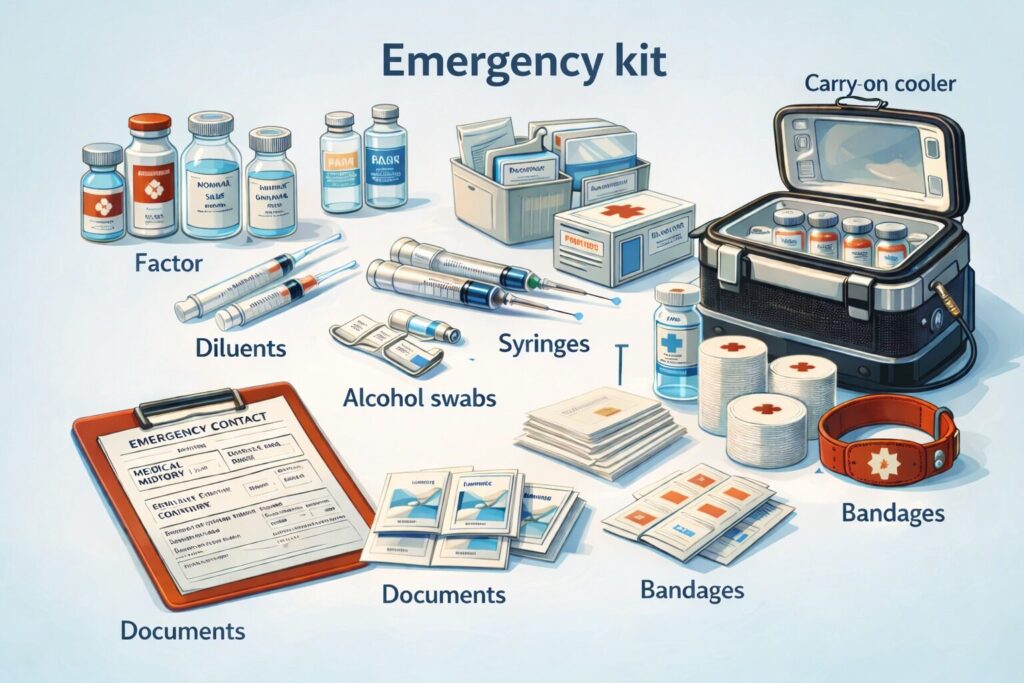
Bleeding emergencies can occur at any time when you’re living with a severe bleeding disorder. Anyone with hemophilia A or hemophilia B is at risk of life-threatening bleeding episodes. Hence, it’s vital to be prepared with an emergency kit that can quickly provide immediate care for either yourself or your loved ones.
Before going on a trip make sure to consult your hemophilia treatment center (HTC) 3 months in advance to adjust schedules. It is recommended to start the prophylactic treatment of factor replacement to avoid bleeding episodes while travelling.
EMERGENCY MEDICAL KIT
These are few of the essentials that you might want to pack if you are travelling
HEMOPHILIA FEDERATION OF INDIA

The Hemophilia Federation (India) (HFI) is a national non-profit organization dedicated to improving the lives of people with hemophilia and other bleeding disorders across India.
HFI promotes early diagnosis, comprehensive care, and standardized treatment protocols through collaboration with treatment centers and government health authorities in providing factors at subsidized rates and creating awareness programs, patient education camps, and training workshops for healthcare professionals. The federation also provides psychosocial support, counseling, and community networking for patients and families thereby creating a more sustainable and safer environment for hemophiliacs.
Hope Beyond Hemophilia
Hemophilia is a lifelong condition, but with timely diagnosis and modern treatment, patients can lead fulfilling and productive lives. Early intervention, regular follow-up, and patient education remain the cornerstones of effective management. Considering the advances made in the field of factor replacement therapy and comprehensive care, the quality of life of hemophiliacs has drastically improved ensuring not only better health outcomes but also dignity and hope for every patient. Equally important is the emotional and social support provided by family, healthcare professionals, and the community. With awareness, compassion, and continued medical progress, individuals with hemophilia can pursue their aspirations with confidence.
References:
- Understanding Hemophilia: Cleveland Clinic. 2024. “Hemophilia.” Cleveland Clinic. https://my.clevelandclinic.org/health/diseases/14083-hemophilia
- Genetics: Centers for Disease Control and Prevention (CDC). How hemophilia is inherited. Atlanta (GA): U.S. Department of Health & Human Services; Available from: https://www.cdc.gov/hemophilia/testing/how-hemophilia-is-inherited.html
- Types of Hemophilia: Fortis Healthcare. Types of Hemophilia explained. Fortis Healthcare; 2025 Nov 26. Available from: https://www.fortishealthcare.com/blogs/types-hemophilia-explained
- Hemophilia in women: Centers for Disease Control and Prevention (CDC). Information for women about hemophilia. Atlanta (GA): U.S. Department of Health & Human Services. Available from: https://www.cdc.gov/hemophilia/about/information-for-women.html
- Hemophilia in pregnancy: Sharma V, Khalid A, Cohen AJ. Management of pregnancy in a patient with severe hemophilia type A. AJP Rep. 2013 Dec 31 ;3(1):29–32. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC3699150/
- Travelling with Hemophilia: Centers for Disease Control and Prevention (CDC). Travel safely with hemophilia. Atlanta (GA): U.S. Department of Health & Human Services. Available from: https://www.cdc.gov/hemophilia/travel-safe/index.html