

Ever felt like you’ll never get rid of the constant, frustrating pain in your back and legs? That no amount of Move or Volini spray will make the dull, nagging ache go away — so much so that you’ve completely adjusted your life around living with it? Well, the relief to your problem might be just one simple vitamin away: Vitamin D. This article aims to shed light on this wonder vitamin— its vital role in the body, the unique functions it performs in women, when and why deficiency occurs, how to recognize its early warning signs, and finally, how to prevent and effectively manage this condition.
Vitamin D – What is it and why do we need it?
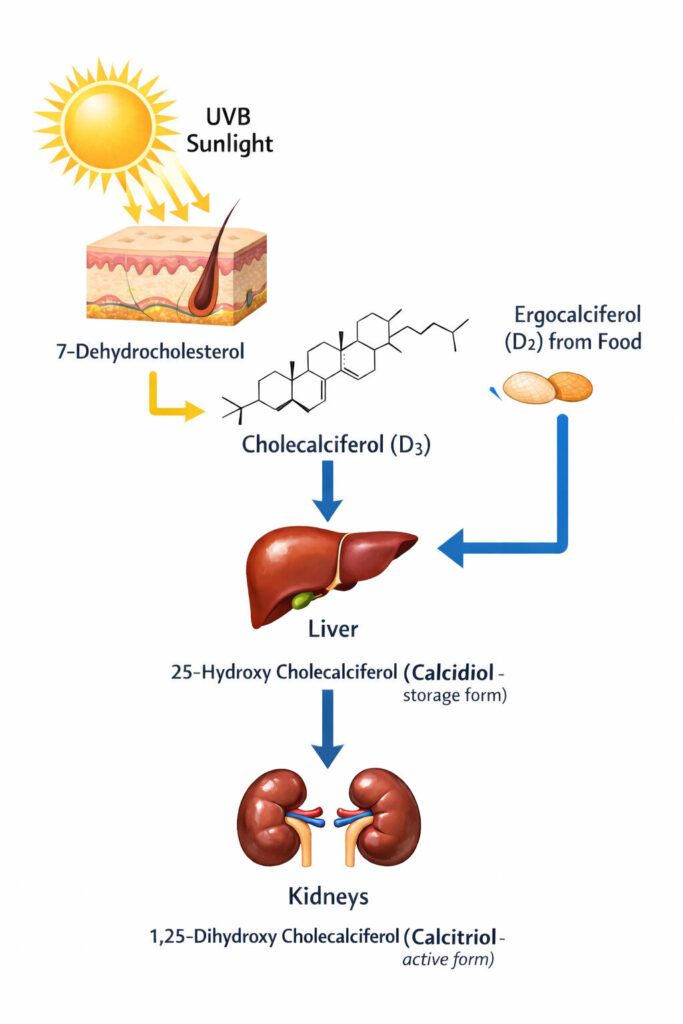
Did you know that vitamin D is not strictly a vitamin at all? It does not necessarily have to come from our diet. In the skin, exposure to adequate UV rays converts an intermediate of cholesterol production (called 7-dehydrocholesterol) into an unstable compound that quickly changes its structure to form cholecalciferol — Vitamin D in its storage form. After this, through activation in the liver and kidneys, it is converted into calcitriol (Vitamin D₃), the active form in the body.
Years of research and debate eventually led to the realization that vitamin D is, in fact, a hormone. Like a hormone, vitamin D has several receptor-mediated functions in the body, the most important being the regulation of calcium levels in the blood — its classical action. As a dynamic hormone, calcitriol plays a dual role: it stimulates bone resorption when blood calcium is low and promotes bone formation when calcium is sufficient. It also increases calcium absorption from the intestines and reduces calcium loss in urine by acting on the kidneys.
Even more intriguing are the non-classical actions of vitamin D. Through mechanisms that are not yet fully understood, higher-than-normal levels of vitamin D have been shown to reduce the risk of prostate and colon cancer. Its anti-inflammatory effects can also help improve pre-diabetes and protect against metabolic syndrome — a condition marked by abnormal cholesterol levels, obesity, and high blood pressure.
Role of vitamin D in women –
- Specifically looking into women’s health, studies show that those with calcidiol (the intermediate form of vitamin D) levels above 20 ng/dL had about a 50% lower risk of developing breast cancer.
- In younger women, vitamin D deficiency is associated with irregular and painful menstrual cycles.
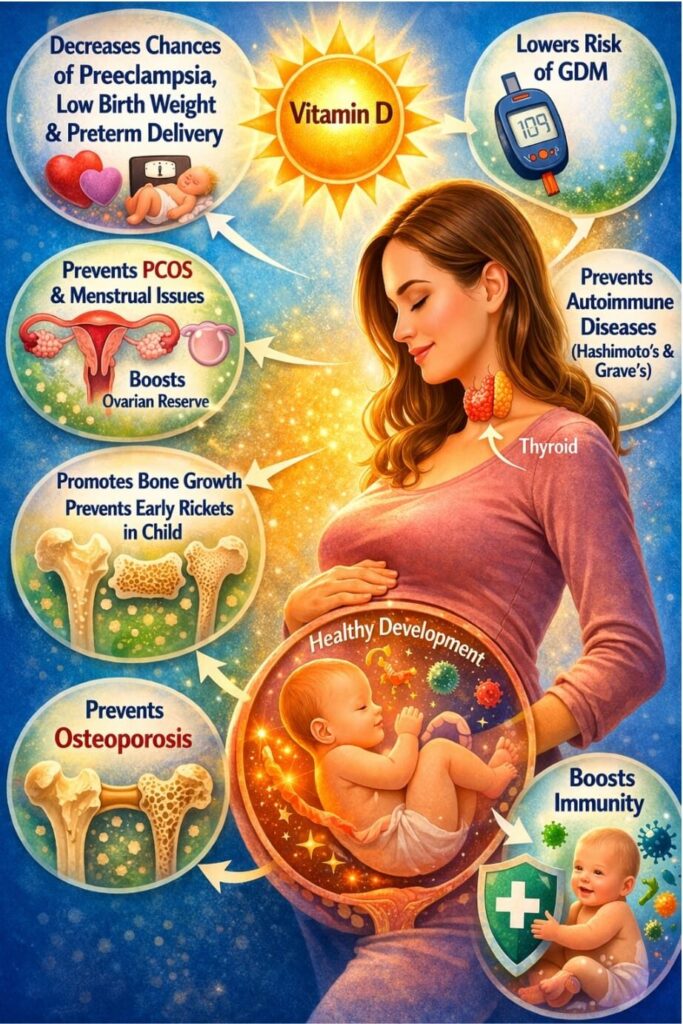
- Low vitamin D levels may also be linked to pregnancy-related complications such as preeclampsia, gestational diabetes, and preterm birth, to name a few.
- In postmenopausal women, adequate vitamin D levels improve bone strength and significantly reduce the risk of fractures.
- Long term deficiency of vitamin D has also proven to worsen autoimmunity in Hashimoto’s thyroiditis and seems to be indirectly linked with other hyperthyroid disorders ( such as Grave’s disease) as well.
Vitamin D deficiency – The silent reason behind your bone pain
Vitamin D – normal levels:
As the saying goes, to understand what is abnormal, we must first understand what is normal. When it comes to vitamin D, doctors measure the level of 25-hydroxyvitamin D (25-OH vitamin D) in the blood. This form, also called calcidiol, is the most stable and abundant storage form in the body, making it the best indicator of overall vitamin D status. As per the Indian Council of Medical Research (ICMR), the following table gives the reference levels of vitamin D accepted by clinicians in India:
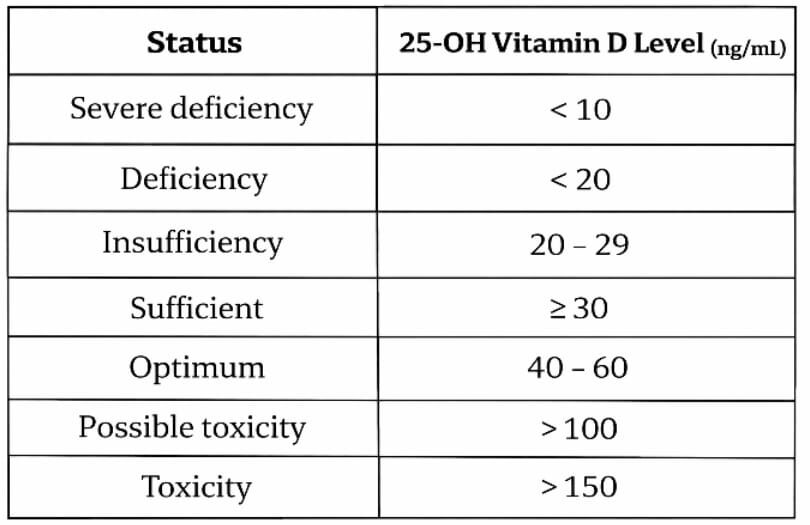
Many clinicians consider levels between 40 and 60 ng/ml to be optimal. In this range, the body not only maintains strong bones but may also benefit from vitamin D’s additional roles, including immune regulation, anti-cancer and anti-inflammatory effects.
Brief overlook of deficiency:
When levels fall into the insufficiency range, symptoms are often subtle. A person may feel more tired than usual or experience mild back and joint discomfort. However, these symptoms are often overlooked. As levels decline further into deficiency, symptoms become more noticeable. These may include persistent bone and joint pain (often affecting the thighs and arms), muscle weakness, increased risk of fractures, and slower wound healing.
Causes of vitamin D deficiency:
As of 2024 – 2026, as per reports from the World Health Organisation (WHO), Vitamin D ranks first among the most common vitamin deficiencies. This is surprising, given that it doesn’t really have to be a part of the diet, as a 5 to 30 min exposure to sunlight between 10:00 am and 3:00 pm two to three times a day is usually enough to meet requirements. The culprit for this is the changing modern lifestyle, and women, particularly housewives, are most susceptible to this.
Environmental and biological factors further limit vitamin D production. Cloudy weather, air pollution, and living in higher latitudes reduce UV-B radiation reaching the skin. Clothing that covers most of the body also decreases exposure. Skin tone plays an important role as well. Darker skin contains more melanin, a natural pigment that protects against harmful ultraviolet radiation. While this protection lowers the risk of DNA damage and skin cancer, it also reduces UV-B penetration, meaning individuals with darker skin need longer sun exposure to produce adequate vitamin D.
Applying sunscreen – especially higher SPF ones (30-50 SPF) – was thought to be another risk factor leading to Vit D deficiency earlier, since it’s known to block entry of UV-B radiations into the skin. While this might sound correct in theory, it is, however, a misconception. Recent studies show that even regular sunscreen application never actually causes clinically significant vitamin D deficiency. This is due to infrequent application, applying in patches and missing areas on the skin through which UV-B rays still enter.
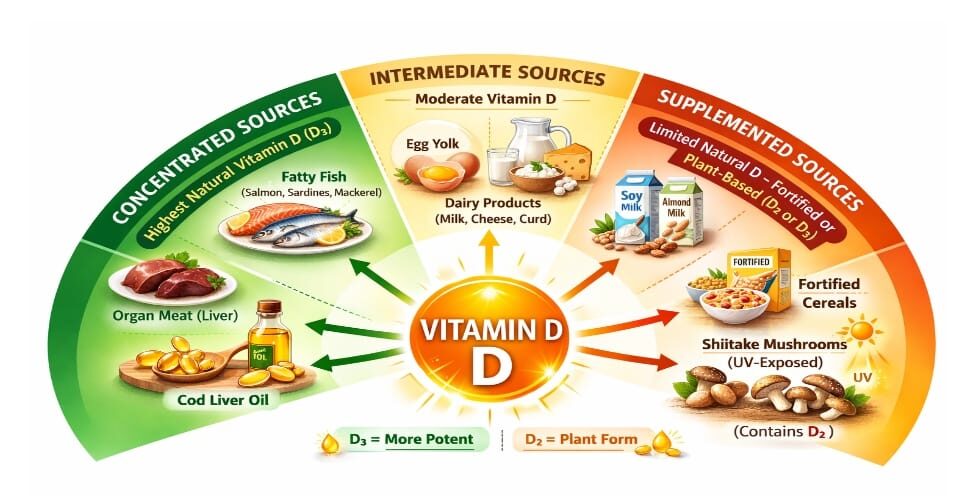
As it’s clear that exposure to sunlight is highly inconsistent, Dietary vitamin D is the only source for most people. However, this is still an issue for vegetarians and vegans, as richest sources are mostly animal-derived. These include fatty fishes (such as salmon, mackerels and sardines), cod liver oil, egg yolk and dairy products. Vegetarian sources are largely limited to fortified foods like cereals, soy milk, almond milk, UV – B exposed mushrooms (shitake), etc.
Another rare cause for its deficiency is obesity and leading a sedentary life. Besides reduced sun exposure, such a lifestyle is often associated with fatty liver and insulin resistance, both of which impair the liver and kidney’s ability to produce the active form of vitamin D (calcitriol). Furthermore, as vitamin D is fat soluble, more body fat would mean that more of it would be stored in this fat, decreasing the circulating amount in the bloodstream. Recent research also suggests that people who have developed liver cirrhosis, those on seizure medications like barbiturates and other medications like rifampicin, clotrimazole are also at risk of its deficiency.
Vitamin D deficiency: Early and late signs and symptoms
Barring a small exception, most studies say that women are far more likely to develop Vitamin D deficiency symptoms than men. Broad global analyses suggest that females are 1.2 to 1.5 times more prone to have low vitamin D levels (<30ng/ml) as compared to males. While symptoms of deficiency remain similar between both genders by and large, in women, osteoporosis and bone fractures often accompany bone aches, particularly at the perimenopausal period. This is a result of the dropping estrogen levels and hormonal changes occurring at this time.
Early Signs:
It’s important to pick up the early signs of vitamin D deficiency, so that it can be detected and treated promptly before full-fledged manifestations start occurring.
Fatigue:
The fatigue experienced is often described as a generalised “heaviness”, especially while climbing up the stairs or getting up from a chair. This is because calcium levels in the blood, which is controlled by vitamin D, also determine how muscles contract in the body.
Bone pain:
The bone pain in the early stages is of a dull and aching type ; diffuse in the sense that it’s difficult to pinpoint a location. Weight bearing bones are usually affected. The pain may improve upon rest but usually never completely subsides. Less common symptoms in this stage are mood swings and depression, which is often mistaken for menopausal changes in women.
Since such symptoms seem very trivial, they’re often ignored particularly by women who juggle a lot of work at home and their job. However, it is this constant ignorance that may result in a major fracture or an excruciating back ache one day, at which point recovery becomes a long and painful journey ahead.
Late signs:
Osteomalacia (in adults):
As vitamin D levels further decline, symptoms further aggravate. With insufficient vitamin D to push calcium into the bones to maintain bone rigidity, bones become very weak, painful, soft and get fractured even in response to minor injuries (pathological fractures). Usually, the lower back, hips and the legs bear the brunt of it. Joints become painful and stiff. Muscles become extremely weak, start twitching and develop spasms. There is a continuous pain and fatigue which never goes away. This disease is called osteomalacia, which is commonly seen in adults. With lowering estrogen levels, perimenopausal women are more adversely affected.
Rickets (in children):
In children, as the bones are still growing, we observe rickets, a disease where only the cartilage-like foundation for the bone is formed, without any calcium salts getting deposited on it, which is like the bone’s cement. As a result the legs bow unable to bear the body weight, and the knees knock each other while walking. Children also suffer from delayed teeth eruption and weak teeth, bead – like swellings on either sides of the breast bone (rachitic rosary), the depression below the lower most rib becoming very prominent (Harrison’s sulcus), softening of the skull bones (craniotabes) and protruding breast bone (Pectus carinatum) . They may also become irritable and refuse to feed.
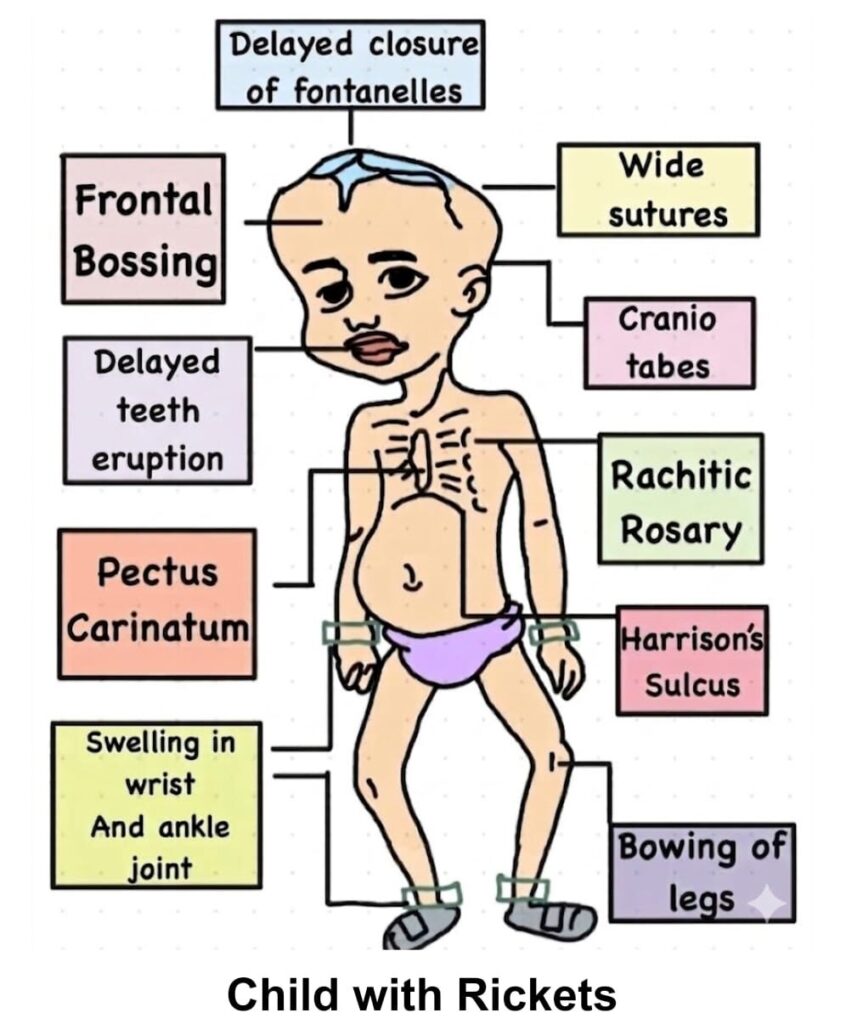
Child with Rickets
In women:
In the later stages, coupled with menopausal changes, women in their forties and fifties are more likely to develop anxiety, depression, mood swings, hair loss and increased susceptibility to infections like influenza.
Vitamin D and women specific concerns
Continuing efforts to understand the true potential of vitamin D have shown that it has a wide range of functions, many influencing women’s health. However, conclusive evidence is still lacking for several roles.
Vitamin D and Osteoporosis:
As women age beyond 30 years, estrogen levels decline. This hormone prevents bone resorption and maintains bone density. When combined with vitamin D deficiency, calcium deposition and bone formation are impaired. This leads to osteoporosis—a condition of reduced bone mineral density, initially causing weakness and pain (osteopenia), and later increasing fracture risk, especially around menopause.
Vitamin D and Female Reproductive Health:
Research shows that women with vitamin D levels above 30 ng / ml have more regular menstrual cycles, higher rates of conceiving, higher reserve of follicles in their ovaries, and decreased chances of developing reproductive disorders like endometriosis, polycystic ovarian syndrome (PCOS) and so on. As a matter of fact, women with healthy vitamin D levels have a much higher IVF success rate than their counterparts. Additionally, it also helps in quality sperm production in males. By regulating the production of sex hormones in the body, vitamin D offers the above mentioned benefits.
During pregnancy, it has been proven that complications like gestational diabetes mellitus (GDM), preeclampsia, post partum hemorrhage (PPH) and low birth weight are higher in women with low vitamin D levels. Optimum vitamin D in the mother also ensures proper bone development in the fetus, decreases the risk of infections immediately after birth and chances of development of rickets in the stages of early childhood.
Vitamin D and thyroid disorders:
Vitamin D strongly modulates the immune response in our body. Not only does it protect our body by fighting disease causing organisms, but it also prevents our immune system from attacking our own body cells (autoimmunity). This is why most people with Hashimoto’s thyroiditis (an autoimmune disorder where the thyroid hormone synthesis is impaired) have very low vitamin D levels. In another autoimmune disease called Grave’s disease, the thyroxine synthesis is higher than normal, and is also associated with low vitamin D levels in 60 – 70 % cases. Low vitamin D3 levels are usually associated with increased circulating levels of TSH in the blood, the hormone that directly controls the functioning of the thyroid gland. Higher the TSH levels over a long period of time, higher are the chances of developing autoimmunity.
Vitamin D and immunity :
While vitamin D plays a strong role in preventing the development of autoimmunity (which, as already known, affects women far more commonly than men), optimum levels of vitamin D in women also helps the immune system fight against respiratory tract and urinary tract infections. The hormone specifically recruits immune cells to the site of infection, and minimises exaggerated inflammatory response at the same time. During pregnancy, vitamin D enables immune adaptation, protecting both the mother and the child this way.
Preventing and treating vitamin D deficiency : The road to optimum health
There is no doubt that vitamin D is a wonder nutrient. Not only does it maintain normal bone health, but it also offers several additional benefits at higher, optimal levels. Therefore, it is crucial to maintain adequate vitamin D levels, especially for women. This can be achieved in the following ways:
- Adequate sunlight exposure: At least 5–30 minutes of exposure between 10:00 am and 3:00 pm, involving the hands, legs, and face, on a sunny day is essential. Sunscreen has minimal impact on this process. However, due to practical limitations, alternative sources are often needed.
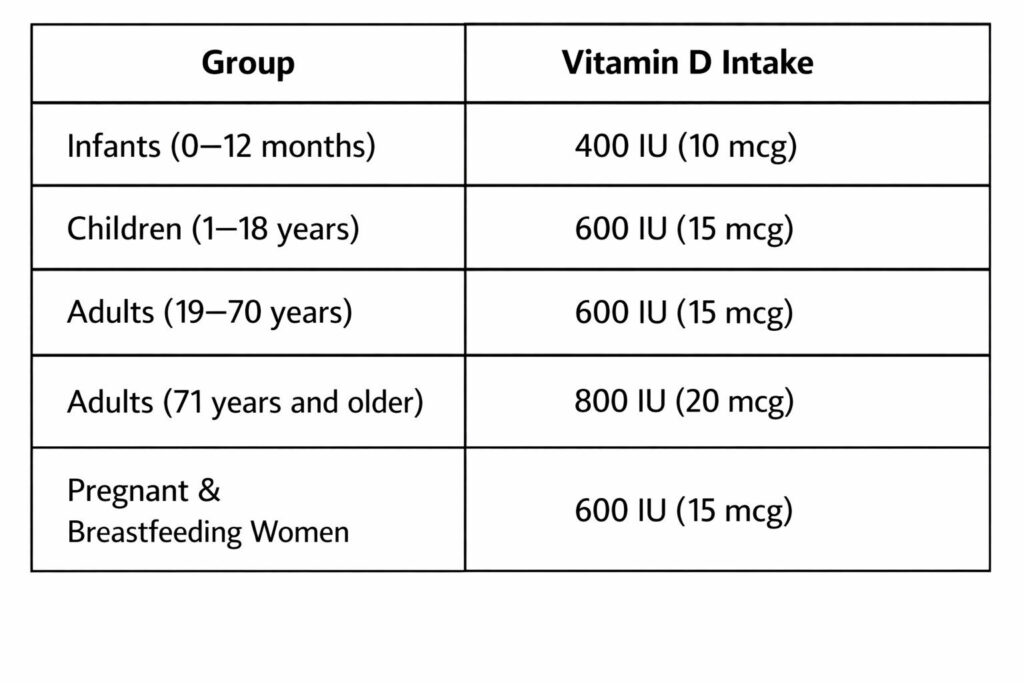
- Consumption of vitamin D–rich foods: For vegetarians, this includes 1–2 glasses of milk daily, 1 cup of fortified yogurt or paneer, and fortified mushrooms when possible. For non-vegetarians, fatty fish like salmon and mackerel (2–3 times a week) and 2–3 eggs per day are good sources. However, a diet alone without sunlight is usually insufficient, and such diets may not be feasible for everyone. The following table shows the recommended daily allowance of vitamin D in different age groups:
- Vitamin D supplements: Many supplements are available, with low-dose vitamin D3 (cholecalciferol) found in over-the-counter multivitamins and syrups. Higher-dose preparations like Uprise-D3, Arachitol, and Calshine are usually prescribed by doctors.
- Nutritional supplements: Women’s Horlicks Plus is a milk-based drink containing calcium, vitamin D, and vitamin K2 in recommended amounts. It has been shown to improve bone health in perimenopausal women over six months.
However, it is relatively expensive, contains high sugar levels (unsuitable for diabetics), and may not be palatable for everyone. Importantly, such products are only supplements and should not replace natural sources.
- Vitamin D injections:Used in cases of severe deficiency (e.g., rickets or osteomalacia) or poor oral tolerance. Intramuscular cholecalciferol is commonly given as a single dose, raising 25-OH vitamin D levels over 12–24 weeks. Alternatives include ergocalciferol and calcitriol, depending on the cause.
- Seeking medical care: Although prevention is better than cure, one must also know when to seek proper medical attention if prevention fails. When patients develop severe bone pain, repeated fractures, children suffer from delay in attaining growth milestones and none of the symptoms show significant improvement even after ensuring adequate sunlight exposure and consuming vitamin D rich food, it becomes imperative to consult a general practitioner, or even better, an orthopedician.
While most cases involve a simple laboratory workup to detect low calcium and vitamin D3 levels in the blood, which is followed by calcium and vitamin D supplementation for 2 months, severe and recurrent cases might also require a through history to rule out medication incompliance, extensive laboratory workup to rule out vitamin D resistance, chronic kidney and liver disease, and comprehensive treatment focussing on vit D supplementation for 2 to 3 months (in the active form as calcitriol in case of resistance) , lifelong calcium therapy, physiotherapy, lifestyle changes and prevention of falls.
- Long-term maintenance: A combination of adequate sun exposure (~20 minutes daily), a vitamin D–rich diet, and supplements when necessary is ideal. Regular monitoring through blood tests every 3–6 months and maintaining physical activity are also important.
CONCLUSION:
Vitamin D is far more than just a nutrient—it functions as a vital hormone that plays a central role in maintaining bone health, regulating calcium balance, and supporting immunity. Its importance becomes even more pronounced in women, where it influences menstrual health, fertility, pregnancy outcomes, and protects against osteoporosis, especially during the perimenopausal and postmenopausal periods.
Despite its significance, deficiency is extremely common due to modern lifestyles with limited sun exposure, dietary insufficiency, and factors such as skin pigmentation, pollution, and sedentary habits. Early warning signs are often subtle—fatigue, vague bone pain, and muscle weakness—and are frequently ignored until more serious complications like fractures, osteomalacia, or metabolic disturbances develop.
Recognizing these early symptoms is crucial for timely intervention. Prevention and management require a balanced approach: regular and safe sunlight exposure, inclusion of vitamin D–rich foods, and supplementation when necessary. In severe cases, medical treatment may be required. Long-term maintenance through lifestyle modification, periodic monitoring, and awareness is key. Ensuring optimal vitamin D levels is not just about preventing deficiency—it is about promoting overall health and improving quality of life, particularly in women.