
When a person usually complains of severe heartburn for a few weeks, we often consider it as “gastritis”, but the true truth lies deeper than we think.
Stick around to know the possible underlying condition to what we call “GERD”.

Introduction
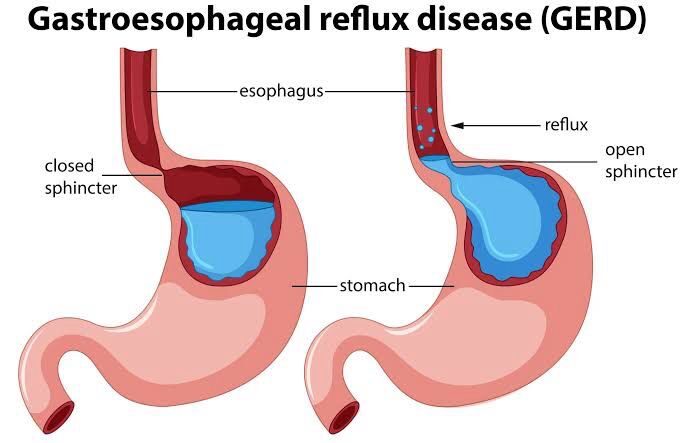
Gastroesophageal reflux disease (GERD) is a condition in which there’s backflow of stomach contents into the esophagus or beyond into other regions, eg, oral cavity, larynx, or the lungs, occurs, primarily resulting in inflammation of the esophageal mucosa.
This condition is considered one of the most common diseases encountered by gastroenterologists and physicians.
The pooled prevalence of GERD in the Indian population is 15.6 (95% CI 11.046 to 20.714).
Risk Factors

These individuals are at an increased risk of developing GERD. The risk factors include:
- Male sex
- White ethnicity
- Age 50 or older
- Tobacco use
- Alcohol consumption
- Delayed gastric emptying
- Use of aspirin and other non-steroidal anti-inflammatory drugs
- Use of drugs that reduce the lower esophageal sphincter pressure, including nitrates, calcium channel blocker agents, anticholinergics, α-adrenergic agonists, theophylline, and morphine
- Anxiety and depression, although the relationship with GERD may be bidirectional.
Multifactorial Origins of GERD
Gastroesophageal Anatomy
Anatomical structures regulate esophageal function and minimize gastroesophageal reflux (backflow). A complex valvular mechanism at the esophagogastric junction resists positive abdominal pressure and negative thoracic pressure. This anatomical mechanism comprises the following structures:
- Lower esophageal sphincter: This physiological sphincter measures 3 to 5 cm long. The high resting tone of the smooth muscle in the lower esophageal sphincter prevents regurgitation of gastric contents into the esophagus.
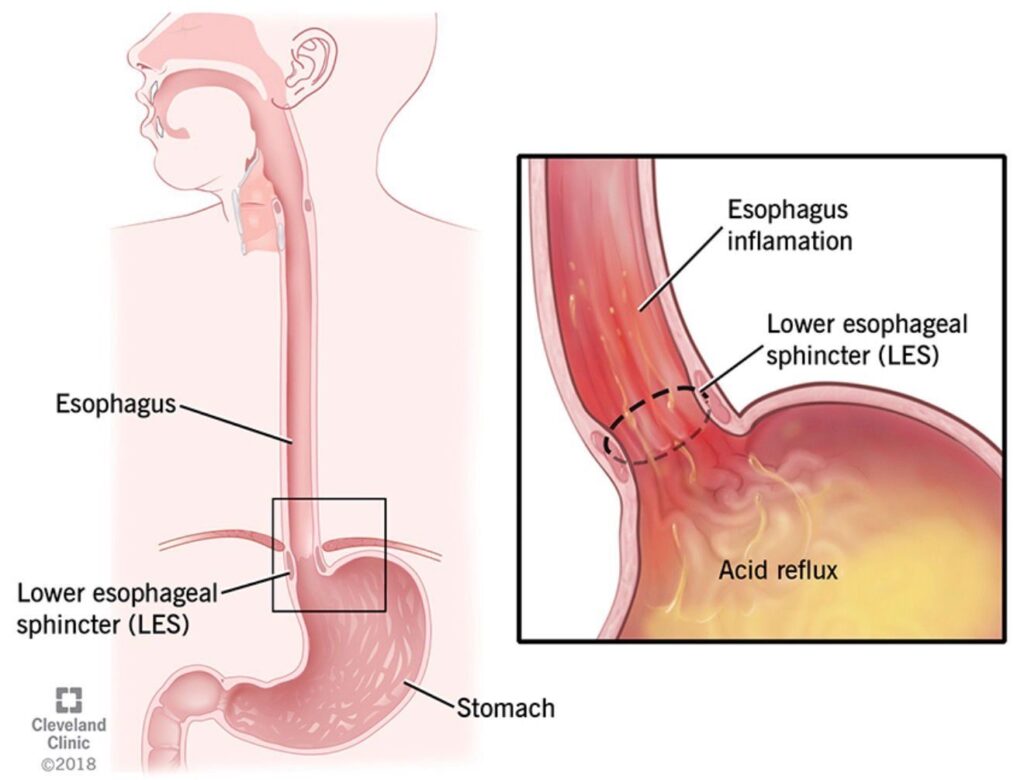
- Diaphragm: The esophagus enters the abdominal cavity through the diaphragmatic hiatus. The diaphragm provides extrinsic reinforcement to the lower esophageal sphincter.
- Abdominal portion of the esophagus: This esophageal segment is exposed to positive intra-abdominal pressure and collapses without a bolus. This collapse provides further support to the lower esophageal sphincter.
- The angle of His: This is the acute angle between the esophagus and the gastric fundus, which enhances the function of the lower esophageal sphincter.
- Phrenoesophageal membrane: This is a fibroelastic ligament that continues the transversalis fascia, which leaves the diaphragm and surrounds the esophagus.
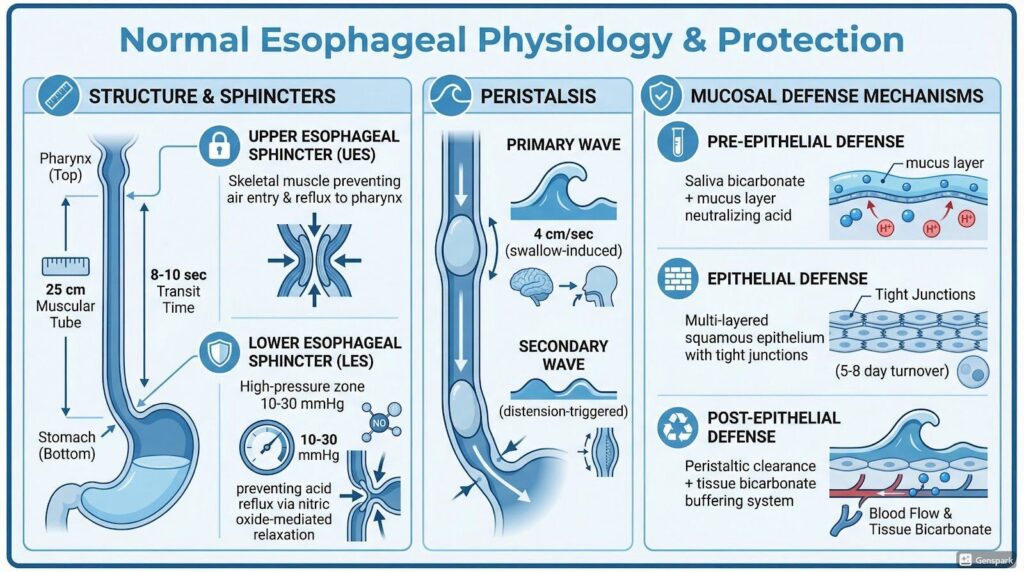
Gastroesophageal Physiological Mechanisms
Physiological mechanisms also protect against gastroesophageal reflux (backflow), including:
- Esophageal motility: Esophageal peristalsis promotes the return of regurgitated acid to the stomach.
Esophageal peristalsis is a vital component of the body’s natural anti-reflux mechanism, acting as a “clearing” mechanism that returns refluxed gastric acid and digestive contents from the esophagus back into the stomach. This process prevents prolonged exposure of the esophageal mucosa to acid, which is the primary cause of esophageal inflammation and damage (esophagitis).
In Gastroesophageal Reflux Disease (GERD), this protective mechanism is often compromised due to Ineffective Esophageal Motility (IEM). When peristalsis is weak or absent:
- Refluxed acid stays in the esophagus longer (prolonged clearance time).
- Acidic contents, bile, and pepsin cause more damage to the esophageal lining.
- Severe cases of GERD are often associated with a failure of the secondary peristaltic response.
- Saliva production: Swallowed saliva contains bicarbonate and is slightly alkaline; salivary mucins also act as lubricants.
- Esophageal epithelial protection: Esophageal submucosal glands also secrete bicarbonate and mucin to protect the distal esophageal mucosa from acidic stomach contents.
Etiologies of Gastroesophageal Reflux Disease
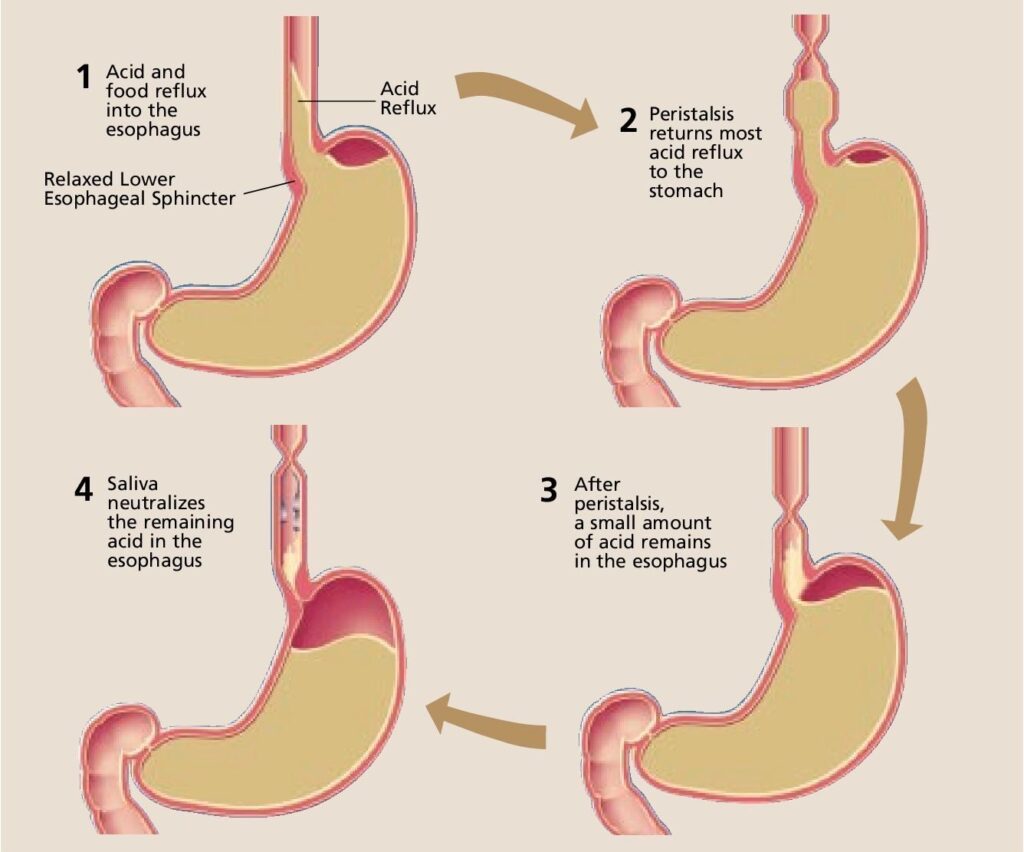
The reflux of gastric contents into the esophagus in healthy individuals is limited, and the refluxed contents are cleared through esophageal peristalsis,as mentioned in the earlier section. However, patients with GERD cannot clear these refluxed contents adequately or produce protective physiological mechanisms. Some of the underlying etiologies of GERD include:
- Transient relaxation of the lower esophageal sphincter or a low resting lower esophageal sphincter pressure
- Hiatus hernia
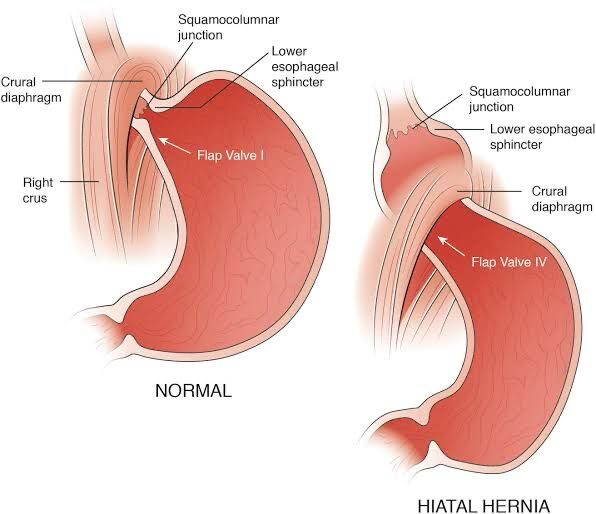
A hiatal hernia is a common condition characterized by the abnormal protrusion of the upper part of the stomach or other internal organs through the diaphragm’s hiatus.
- A lax hiatus may lead to gastroesophageal reflux disease.
The development of a hiatal hernia is multifactorial, with contributing factors including
1.congenital anatomical defects, increased intraabdominal pressure (as seen in obesity, pregnancy, and chronic coughing)
2. Age-related changes in the diaphragm’s muscle tone.
- Extrinsically increased intra-abdominal pressure, as in obesity
- Intrinsically increased intra-abdominal pressure, as observed during pregnancy or in patients with high-volume ascites
- Impaired esophageal motility
- Impaired saliva production
- Impaired esophageal mucosal defense mechanisms
Normal Gastroesophageal Physiology
Pathophysiology
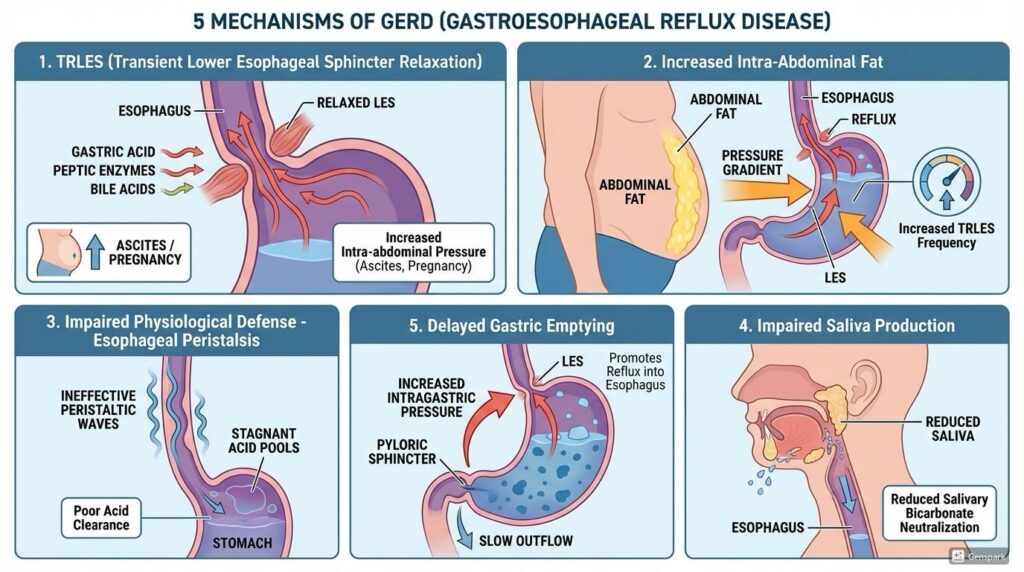
The following pathophysiological mechanisms underlying GERD are related to the etiological causes:
- Transient lower esophageal sphincter relaxation (TRLES): This change results in regurgitation of the gastric acid, peptic enzymes, and bile acids into the esophagus. The effect is enhanced in patients with increased intra-abdominal pressure, such as patients with ascites and pregnant women. TRLES is the most common mechanism explaining reflux in normal individuals and those with GERD.
- Increased intra-abdominal fat: This change increases the gastroesophageal pressure gradient and the frequency of the TRLES phase, leading to the reflux of gastric content into the esophagus.
- Impaired physiological defense mechanisms: Dysregulation of esophageal peristalsis could lead to ineffective clearance of acids from the lower esophagus.
- Impaired saliva production: The process of neutralizing the acids refluxed into the esophagus decreases.
- Impaired esophageal mural defense mechanisms
- A compromised pre-epithelial barrier comprises an unstirred water layer combined with bicarbonate from swallowed saliva and the secretion of submucous glands.
- Impaired epithelial defense mechanisms typically include tight intercellular junctions, cellular and intercellular buffers, and cell membrane transport proteins.
- Reduced blood supply to the esophagus and other postepithelial lines of defense.
How GERD Affects the Body
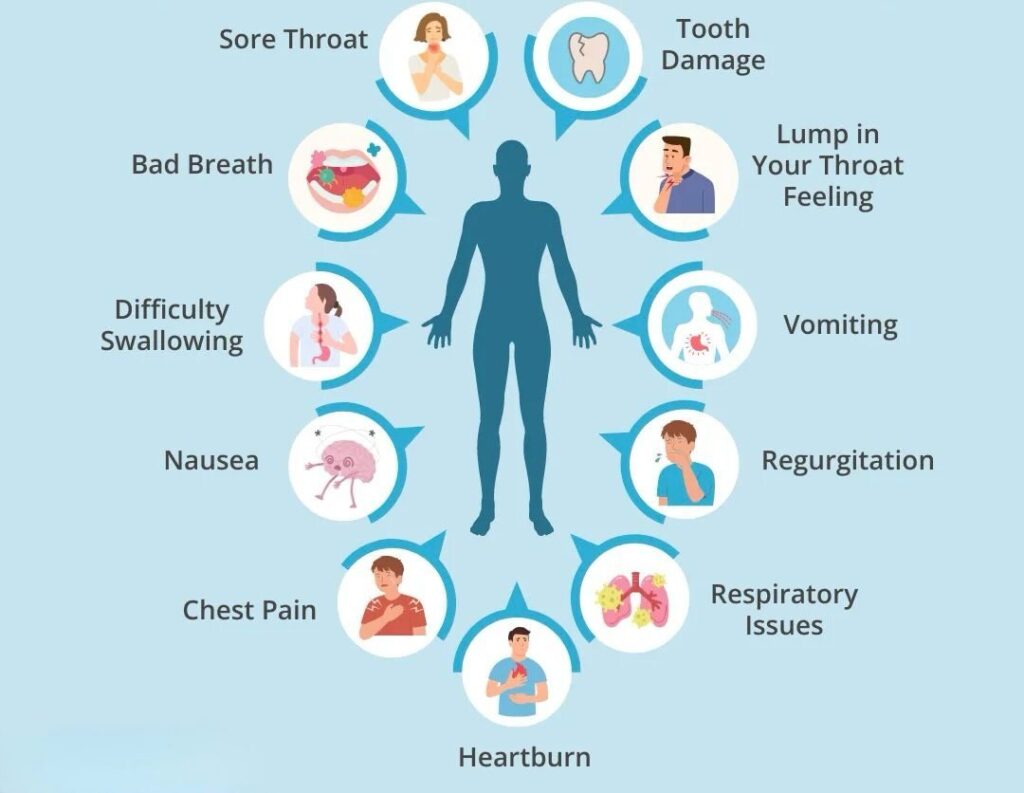
8 key symptoms:
- Heartburn: A burning pain in the chest, often after eating or lying down.
- Regurgitation: Stomach acid or sour liquid coming back up into your throat or mouth.
- Chest Pain: Pain in the chest, sometimes mistaken for heart-related issues.
- Difficulty Swallowing (Dysphagia): Feeling like food is stuck or pain when swallowing.
- Chronic Cough: A persistent dry cough, often without a cold.
- Hoarseness: A rough or raspy voice due to irritation.
- Sore Throat: A raw or irritated throat, especially in the morning.
- Lump in Throat (Globus Sensation): Feeling like a lump is in your throat even when it’s empty.
Underlying conditions that can mimic GERD
- Gastroesophageal Reflux Disease Heartburn or regurgitation is reported weekly by 18-28% of the population, highlighting the prevalence of gastroesophageal reflux disease (GERD).
- Most cases of heartburn result from excess acid reflux, but reflux of weakly acidic or nonacidic fluid can produce similar symptoms.
- Alkaline reflux esophagitis elicits GERD symptoms in patients who have had surgery for peptic ulcer disease.
- 10% of patients with heartburn exhibit no acidic or nonacidic esophageal reflux and are considered to have functional heartburn.
- Most GERD patients do not exhibit esophageal injury, but 5% develop esophageal ulcers.
- Esophageal adenocarcinoma usually complicates prolonged acid reflux.
- 8 to 20% of GERD patients exhibit esophageal intestinal metaplasia, a transformation of the cells in the lining of your upper digestive tract, often the stomach or the esophagus (food pipe),termed Barrett’s metaplasia, which leads to esophageal adenocarcinoma.
How will we know whether it’s GERD or other gut related diseases?
Here’s a list of symptoms that may indicate the above mentioned condition-
- GERD classically produces heartburn, a burning sensation behind the breastbone that moves toward the neck. Heartburn often is worsened by meals and may awaken the patient.
- Associated symptoms include backflow of acid or nonacidic fluid and water brash, the reflex release of salty saliva into the mouth.
- Atypical symptoms include pharyngitis, asthma, cough, bronchitis, hoarseness, and chest pain that mimics angina.
- Some patients with acid reflux on esophageal pH testing note abdominal pain instead of heartburn.
- In atypical GERD, pharyngeal erythema( a red, irritated, and inflamed throat) and wheezing may be noted.
Esophageal reflux may result in complications, including-
- Inflammation of Esophagus(Esophagitis)
- Upper GI( gastrointestinal) bleeding
- Anaemia-Blood having less ability to carry oxygen
- Abnormal narrowing of Esophagus (Esophageal stricturing)
- Difficulty in swallowing(Dysphagia)
- Tissue lining the lower esophagus changes into tissue similar to the intestinal lining (Barrett esophagus)
GERD may also result in extra-gastrointestinal complications, including-
- Tooth erosions
- Inflammation of larynx(laryngitis)
- cough
- asthma
- Inflammation of sinus(sinusitis)
- Idiopathic pulmonary fibrosis.
TREATMENT AND PREVENTION
The physician will tell the patients to try lifestyle changes,the most important change which can only help the patients get better. He might start you with over the counter medicines as a first line of treatment. If you don’t experience relief within a few weeks, then prescription medicine and additional tests may be recommended which has been told earlier.
Treatment options for hiatal hernia range from conservative to surgical approaches, depending on symptom severity and the presence of complications. Conservative measures include dietary modifications, weight loss, and pharmacological therapy to manage reflux symptoms. Surgical repair, such as laparoscopic Nissen fundoplication, is considered for individuals with severe or refractory symptoms or complications like esophagitis or Barrett esophagus.
Lifestyle Modifications:
- Weight loss for overweight patients.
- Elevate the head of the bed by 6-8 inches.
- Avoid eating 2-3 hours before bedtime.
- Avoid trigger foods: Caffeine, chocolate, alcohol, peppermint, fatty/spicy foods.
Medical management of GERD
Focuses on acid suppression, symptom relief, and healing esophageal mucosa, primarily utilizing proton pump inhibitors (PPIs) as the cornerstone therapy e.g., omeprazole ,, Pantoprazole and antacids etc.
[Note- With proper care,right medication,early diagnosis,conditions like GERD can be effectively treated. For the right management,approach a physician as early as possible.]
Surgical Management
Surgery is indicated for patients with refractory GERD, failure of medical management (PPIs), large hiatal hernias, or complications.
Prevention
Avoidance-
- Dietary variables like a non-vegetarian diet
- Mint
- Chocolate
- Acidic foods and beverages include tomatoes, garlic, onions, citrus fruits, and juices.
- Carbonated beverages, such as seltzer or soda.
- Fried foods and spices.
- Caffeinated beverages like tea and coffee.
- Give up smoking and
- Abstain from alcohol.
Need to increase Fiber Content in Diet
Foods high in fiber include:
- Vegetables
- Fruits
- Legumes such as beans and lentils
- Seeds and nuts
- Whole grains, such as quinoa, brown rice, oatmeal, and whole-wheat pasta or bread
GERD AWARENESS WEEK

Occurs annually in late November, established by the International Foundation for Gastrointestinal Disorders (IFFGD) to educate the public about Gastroesophageal Reflux Disease(GERD), its common symptoms, serious risks (including esophageal cancer) and its treatment options.
What’s the purpose of this?
- To raise public awareness about GERD, a prevalent digestive disorder.
- To highlight the daily challenges, physical, and emotional toll on those living with it.
- To emphasize the importance of early diagnosis and management to prevent severe complications like esophageal cancer.
CONCLUSION
I hereby conclude that GERD is more than just a ‘normal’ gastritis, yet many people delay seeking professional help in favor of self-medication. Because of its potential severity, it is crucial to recognize the symptoms early and consult a physician rather than waiting for the condition to escalate.
References:
Source: Research Journal of Pharmacology and Pharmacodynamicshttps://share.google/nSmZwNYSifxJvydpy)
Epidemiology and symptom profile of gastroesophageal reflux in the Indian population: report of the Indian Society of Gastroenterology Task Force. Shobna J Bhatia et al. Indian J Gastroenterol. 2011 May.
GERD awareness week from aboutgerd.org