

Patient: “AHEM! AHEM!”
Doctor says :”Take this syrup , you will be fine.”
You take it….. and then suddenly …
Ahhh….. relaxation,slight euphoria everything feels so slow and nice.

Cough syrup addiction is a growing public health concern, particularly among adolescents and young adults. Many cough syrups are available over the counter and contain psychoactive substances capable of producing euphoria, sedation, or hallucinations when consumed in excessive amounts. Repeated misuse can lead to psychological dependence, physical complications, and social dysfunction. Among the commonly abused ingredients are dextromethorphan (DXM), codeine, promethazine, diphenhydramine, and antihistamines. The increasing accessibility and perception that these medicines are “safe” because they are medically approved contribute significantly to their misuse.
What is Cough Syrup addiction?
Cough syrup addiction refers to compulsive and repeated misuse of cough medications despite harmful consequences. Individuals may consume cough syrups in doses much higher than recommended to experience euphoria, dissociation, relaxation, or hallucinations. Addiction develops when repeated use alters brain reward pathways, leading to craving, tolerance, and withdrawal symptoms. Some users initially take cough syrups for genuine respiratory symptoms but gradually escalate the dosage for recreational effects. Both prescription-based and over-the-counter cough preparations can be abused.
Commonly Misused Components
What does this “magic syrup” consist of
The components of the usual and misused ones are :
- Codeine (opioid)
- Dextromethorphan (brain acting)
- Antihistamine ( sedation)
So what starts as a relief medication is taken repetitively and eventually leads to Addiction.
Your brain starts perceiving it in a different sense.

The most frequently misused ingredient is dextromethorphan (DXM), a non-opioid antitussive found in many cough and cold preparations. At high doses, DXM acts similarly to ketamine or phencyclidine, producing dissociative and hallucinogenic effects. Codeine-containing syrups are also commonly abused because codeine is an opioid capable of causing dependence and sedation.
Other substances often present in cough syrups include promethazine, diphenhydramine, chlorpheniramine, pseudoephedrine, and acetaminophen. Antihistamines may produce sedation and delirium at high doses, while decongestants can cause stimulant effects. Combination products may therefore increase toxicity and risk of overdose.
Why Does Addiction Occur? (Risk Factors)
Several factors contribute to cough syrup addiction. Easy availability without prescription is one of the major causes. Adolescents and young adults are particularly vulnerable due to curiosity, peer influence, and experimentation. Psychological factors such as stress, anxiety, depression, low self-esteem, and previous substance abuse also increase risk. Social media trends and misconceptions that cough medicines are safer than illicit drugs further promote misuse.
Genetic and biological factors may also influence addiction risk. Individuals with variations in liver enzyme CYP2D6 metabolize DXM differently, resulting in stronger psychoactive effects in some users. Concurrent use of alcohol, cannabis, stimulants, or antidepressants can intensify intoxication and dependence potential.
Mechanism: How It Affects the Brain (Consequences)
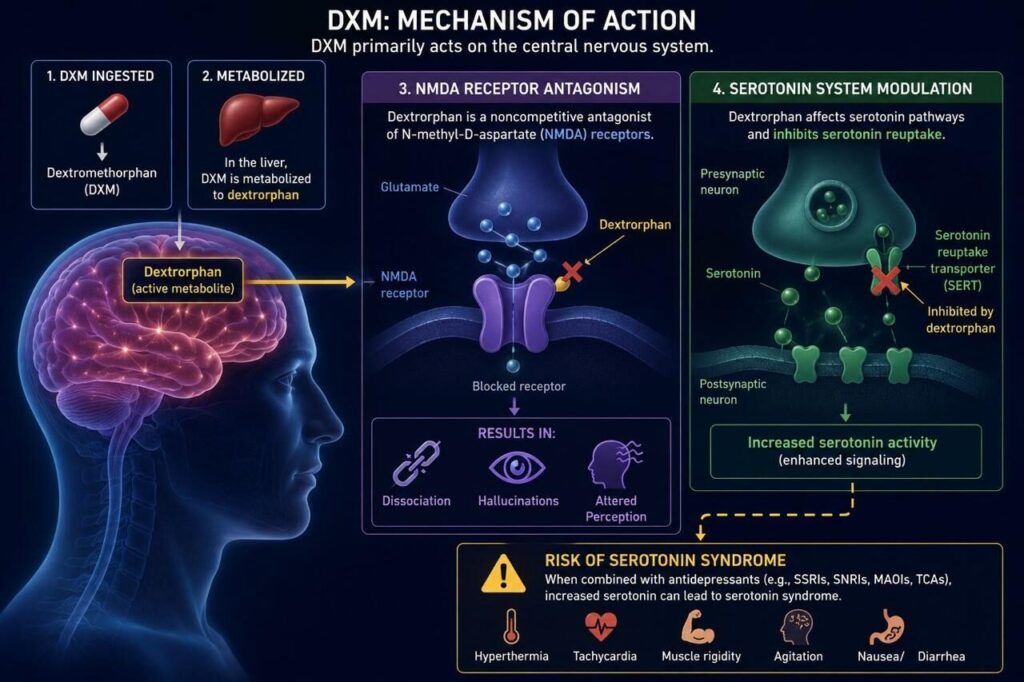
DXM primarily acts on the central nervous system. Its active metabolite, dextrorphan, blocks N-methyl-D-aspartate (NMDA) receptors, leading to dissociation, hallucinations, and altered perception. It also affects serotonin pathways and inhibits serotonin reuptake, which may result in serotonin syndrome when combined with antidepressants.
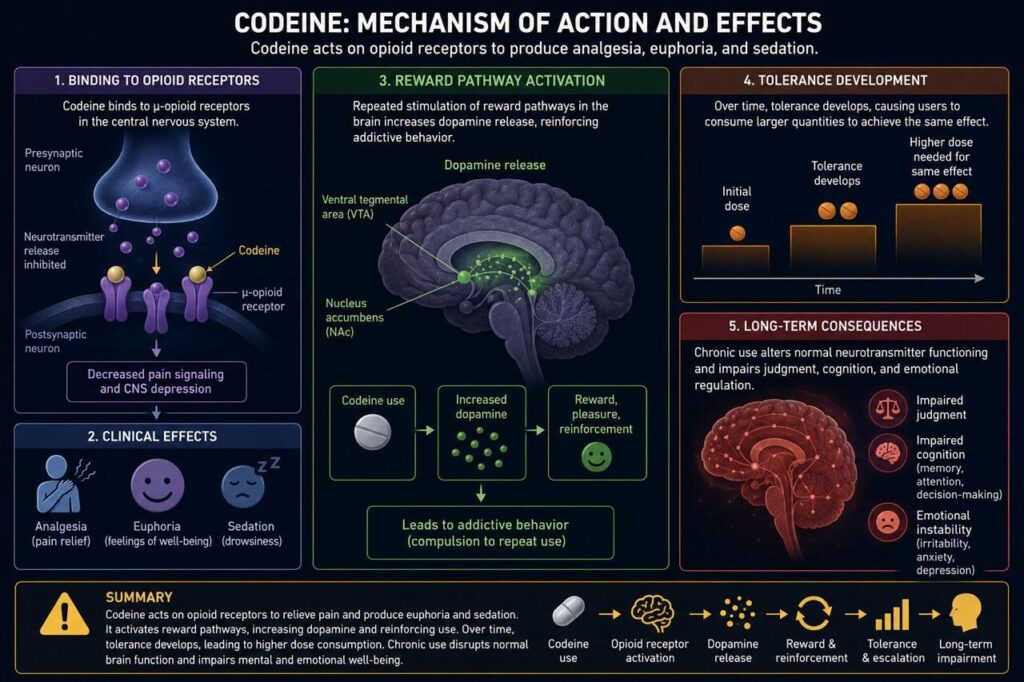
Codeine acts on opioid receptors, producing analgesia, euphoria, and sedation. Repeated stimulation of reward pathways in the brain increases dopamine release, reinforcing addictive behavior. Over time, tolerance develops, causing users to consume larger quantities to achieve the same effect. Chronic use alters normal neurotransmitter functioning and impairs judgment, cognition, and emotional regulation.
Clinical Features (Signs & Symptoms)
Patients with cough syrup addiction may present with behavioral, psychological, and physical symptoms. Common signs include excessive drowsiness, dizziness, slurred speech, poor concentration, confusion, and mood changes. Some individuals exhibit agitation, hallucinations, paranoia, or dissociative experiences.

Physical manifestations may include tachycardia, hypertension, sweating, dilated pupils, nausea, vomiting, tremors, and impaired coordination. Chronic users often show declining academic or occupational performance, social withdrawal, and secretive behavior. Tolerance and withdrawal symptoms such as irritability, insomnia, anxiety, and cravings are common in dependent individuals.
Complications
Affects multiple organs and overall health
- Liver damage – especially with paracetamol/alcohol-containing syrups.
- Respiratory depression – slowed or difficult breathing. (opioids/DXM)
- Cardiac issues – abnormal heart rhythm with high dose/long use.
- Brain damage – due to hypoxia or toxic exposure.
- Cognitive effects – memory loss, confusion.
- Dependence & withdrawal – headache, nausea, sweating, anxiety.
When to Suspect the Addiction (Danger Signs)
Healthcare professionals should suspect cough syrup addiction in individuals requesting frequent refills, consuming unusually large quantities, or presenting repeatedly with unexplained neurological or psychiatric symptoms. Adolescents with sudden behavioral changes, declining school performance, or possession of multiple cough syrup bottles should also be evaluated. A detailed history of substance use and mental health assessment is essential.
1.Using cough 😷 whenever they feel.
2.Taking higher doses than prescribed.

3. Feeling Euphoric after consuming.
4.Hiding bottles or lying about usage.
5.Drowsiness,slurred speech or poor coordination.
6.Poor performance at workplace,school or college.
Management
Management involves both acute treatment and long-term rehabilitation. In overdose situations, stabilization of airway, breathing, and circulation is the priority. Activated charcoal may be considered in early poisoning cases. Naloxone can help reverse opioid-related respiratory depression in codeine toxicity. Agitation, seizures, and serotonin syndrome require supportive care and symptomatic treatment.
Long-term treatment includes counseling, cognitive behavioral therapy, motivational enhancement therapy, and psychiatric support. Treatment of underlying mental health disorders is important. Family education and substance abuse rehabilitation programs improve recovery outcomes.
Prevention & Awareness
Prevention strategies include stricter regulation of cough medicine sales, pharmacist monitoring, public education, and parental supervision. Awareness programs in schools and communities can help educate adolescents about the risks of misuse. Healthcare professionals should counsel patients regarding proper dosage and dangers of recreational use.

How to avoid cough syrup addiction
- Always use as prescribed by doctor, Do not self medicate or extend the treatment period without medical advice.
- Combining cough syrup with alcohol or sedatives increases the risk of addiction and overdose.
- Try opting for non-codeine syrups.
- Read labels properly,check for DMX and codeine ask doctor if they are essential for your condition.
- Educate the teens,many teens get addicted to cough syrup for temporary high.
- Seek medical help before it worsens.
Conclusion
Cough syrup addiction is a serious but preventable form of substance misuse. Ingredients such as dextromethorphan and codeine can produce psychoactive effects leading to dependence and severe health complications. Early recognition, proper medical management, counseling, and public awareness are essential in reducing morbidity and mortality associated with cough syrup abuse. A multidisciplinary approach involving healthcare professionals, families, educators, and policymakers is necessary to address this growing problem effectively.