
Imagine an elderly woman, recently widowed, living alone. She wakes each morning, makes herself a cup of tea, and eats two slices of toast. Lunch, if she manages it, is a few crackers. Dinner is a thin soup. She has lost interest in cooking; there seems little point for one person. Her appetite is diminished, her teeth ache, and the grocery store feels far. Over weeks and months, this becomes her routine. And quietly, without drama, her serum sodium begins to fall.
This is not a rare story. It plays out in homes, nursing facilities, and hospitals across the world, and yet the diagnosis underlying it, tea and toast syndrome, remains absent from most clinical conversations about hyponatremia.
Introduction
Hyponatremia, defined as serum sodium below 135 mEq/L, is the most frequently encountered electrolyte abnormality in clinical practice, with prevalence estimates of 15 to 30% among hospitalized patients and even higher rates in institutionalized elderly cohorts. Its consequences extend far beyond laboratory value. Hyponatremia is independently associated with increased fall risk, bone fractures, cognitive impairment, prolonged hospitalization, and all-cause mortality. A serum sodium of 128 mEq/L is not an incidental finding; it is a clinically significant state that demands explanation.
The elderly are disproportionately affected for reasons that run deeper than coincidence. Aging impairs glomerular filtration, reduces urinary concentrating and diluting capacity, blunts thirst sensation, and alters ADH responsiveness, a convergence of physiological changes that collectively destabilize sodium and water homeostasis. Layered onto this biological substrate are the social realities of aging: grief, isolation, depression, poverty, immobility, and dental disease, all of which erode the quality and quantity of dietary intake. Tea and toast syndrome sits at precisely this intersection.
The syndrome is defined as chronic hyponatremia arising directly from severely restricted dietary solute intake, particularly protein and sodium, leading to insufficient urinary osmole generation and impaired free water excretion. What makes it persistently underdiagnosed is a fundamental gap in clinical evaluation. Standard hyponatremia workups interrogate renal function, thyroid and adrenal axes, volume status, and medication lists. They rarely interrogate what the patient has been eating for the past six months. That omission, modest in its cost to correct, carries significant diagnostic consequences.
Historical Background
Diet-associated hyponatremia was not always a recognized entity. The earliest clinical descriptions emerged from the geriatric and nephrology literature of the 1980s and 1990s, where astute clinicians began noticing a recurring pattern: elderly patients, frequently widowed, socially isolated, and economically marginal, presenting with chronic mild-to-moderate hyponatremia that resolved with nutritional rehabilitation and recurred when dietary context was ignored. The clinical profile was consistent enough to be memorable: malnourished individuals with low BUN, low urine osmolality, and a dietary history revealing near-total absence of protein and salt. The concept gained wider clinical traction through nephrology literature in the late 1990s, with contributions including Thaler’s 1998 work helping formalize low-solute hyponatremia as a distinct mechanistic category, separable from SIADH and requiring its own diagnostic and therapeutic framework.

Epidemiology
Tea and toast syndrome does not distribute randomly. It concentrates predictably in individuals whose social and physical circumstances conspire against adequate nutrition. Elderly individuals living alone constitute the highest-risk group, as loss of a spouse removes not only companionship but frequently the primary architect of household meals. Institutionalized patients in nursing homes and long-term care facilities are similarly vulnerable. Low socioeconomic status and poor dentition compound the risk: an individual who cannot comfortably chew meat or legumes will gravitate naturally toward soft, low-protein alternatives like bread, biscuits, and porridge.
Contributing factors extend beyond the physical. Depression, extraordinarily prevalent and persistently underdiagnosed in the elderly, suppresses appetite and motivation to eat. Cognitive impairment disrupts meal planning. The anorexia of aging, a well-documented physiological reduction in appetite with advancing age, reduces overall intake even in otherwise healthy older individuals. Paradoxically, excessive fluid intake, large volumes of tea, water, or juice consumed in the absence of adequate solute, accelerates the syndrome by increasing the free water load that the solute-depleted kidney cannot handle.
Normal Renal Physiology of Water Excretion
To understand why this syndrome causes hyponatremia, one must first appreciate how the kidney normally excretes water and, critically, what it requires to do so.
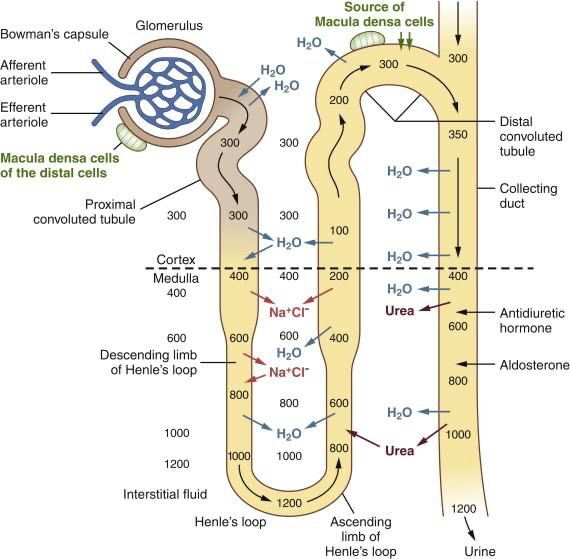
The kidney’s ability to excrete free water is governed by a simple but non-negotiable constraint: to eliminate water in urine, that urine must carry solutes with it. The minimum achievable urine osmolality, the most dilute urine the kidney can produce, is approximately 50 mOsm/kg. This is the physiological floor. Under normal dietary conditions, an adult generates approximately 900 mOsm of urinary solutes daily. The dominant contributor is urea, the metabolic end-product of dietary protein catabolism, with sodium and its accompanying anions contributing substantially as well.
The arithmetic that governs free water excretion is straightforward: maximum daily free water clearance equals total daily osmole load divided by minimum urine osmolality. At 900 mOsm/day and a minimum urine osmolality of 50 mOsm/kg, the kidney can theoretically excrete 18 litres of free water per day. This generous capacity is why a healthy individual can drink several litres of water without developing hyponatremia. The system is robust, but only as long as solute intake remains adequate.
Pathophysiology
In tea and toast syndrome, the solute supply collapses. A diet of tea, toast, and crackers provides only approximately 150 to 200 mOsm of urinary osmoles per day, roughly one-fifth of the normal load. Low protein intake means minimal urea generation. Low sodium intake simultaneously reduces the electrolyte contribution to urinary osmolarity. The osmole pool is depleted from both ends at once.
When the same arithmetic is applied: at 200 mOsm/day, 200 divided by 50 yields only 4 litres of free water that can be excreted daily. If fluid intake exceeds 4 litres, the surplus water has nowhere to go. It is retained, dilutes the extracellular fluid, and serum sodium falls.
The critical and frequently misunderstood point is that ADH is appropriately suppressed in tea and toast syndrome. The hypothalamus correctly senses dilute plasma and inhibits ADH release. The kidney is producing maximally dilute urine. And yet hyponatremia still develops, because even maximally dilute urine cannot carry enough water out of the body when the osmole supply is this limited. This is the defining mechanistic distinction from SIADH, where hyponatremia arises from ADH excess causing inappropriately concentrated urine. In tea and toast syndrome, the urine is dilute; it is the osmole tank that is empty.

Comparison with Related Conditions
Tea and toast syndrome must be systematically distinguished from its closest mechanistic relatives. Beer potomania operates through an analogous mechanism: low solute intake combined with very high fluid intake, ADH appropriately suppressed, and low urine osmolality. The distinction lies in the nature of fluid excess and social context. SIADH differs fundamentally: ADH is elevated or inappropriately non-suppressed, urine osmolality is high, characteristically above 100 and often well above 300 mOsm/kg, and the fractional excretion of uric acid (FEUric acid) exceeds 12%. In tea and toast syndrome, urine osmolality is low and FEUric acid is normal. BUN is low in both tea and toast syndrome and beer potomania owing to poor protein intake, while it is typically normal in SIADH. Psychogenic polydipsia involves normal solute intake with dramatically elevated fluid intake, and the psychiatric context distinguishes this readily.
Clinical Features and Laboratory Findings
The clinical presentation is rarely dramatic, and that is precisely what makes it dangerous. At mild degrees of hyponatremia (sodium 130 to 135 mEq/L), symptoms are nonspecific: anorexia, nausea, fatigue, and malaise, easy to attribute to aging or depression. As sodium falls into the moderate range (125 to 130 mEq/L), cognitive slowing, irritability, and gait instability emerge. Gait disturbance deserves particular attention; even mild hyponatremia significantly impairs postural stability in the elderly, increasing fall risk with downstream consequences including hip fractures and functional decline. Severe hyponatremia below 120 mEq/L can manifest as seizures and coma, though this degree is less common in the typically slow, chronic course of this syndrome.
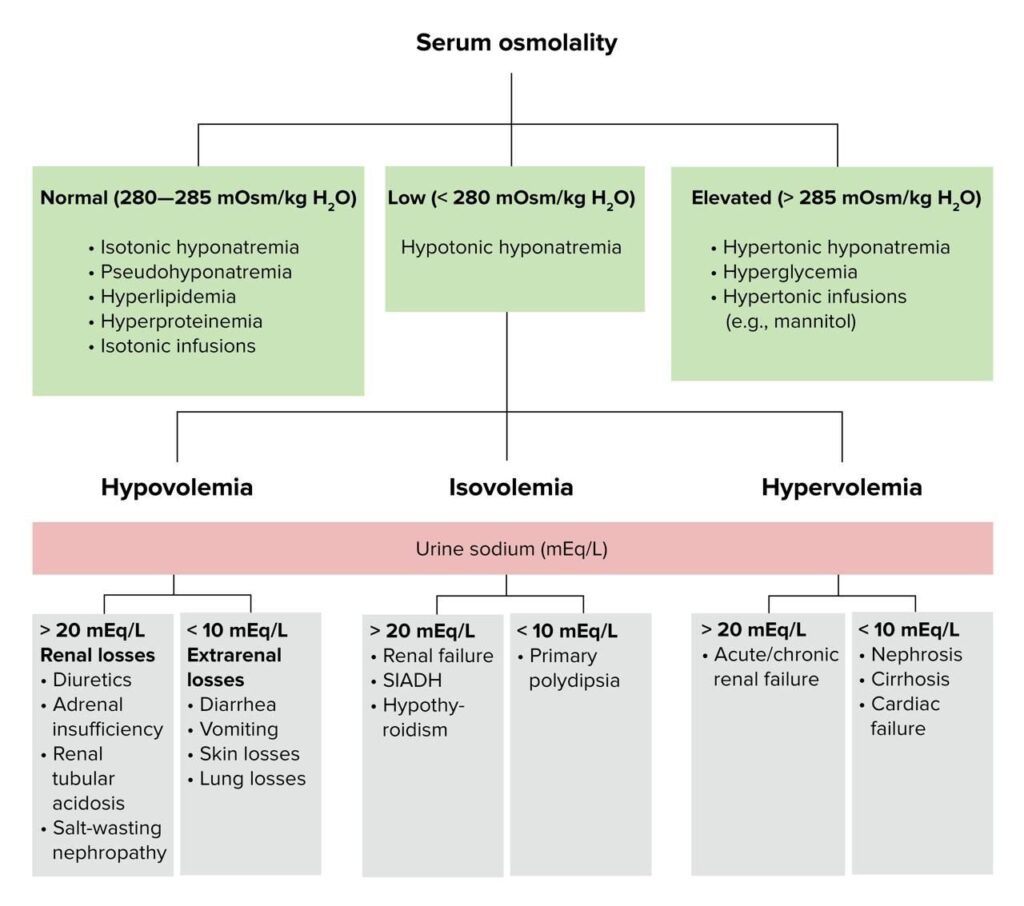
The laboratory profile is coherent and diagnostically instructive when read as a whole. Serum sodium is low. Serum osmolality is correspondingly low. BUN is characteristically low, reflecting inadequate dietary protein rather than renal impairment, making it a useful positive marker for the diagnosis. Serum uric acid may be reduced, and FEUric acid is normal, contrasting directly with SIADH where it is elevated. Urine osmolality is inappropriately low relative to serum osmolality, the opposite of SIADH. Thyroid function and morning cortisol are normal, excluding endocrine contributors. Together, low sodium, low BUN, low urine osmolality, normal FEUric acid, and normal endocrine function in an euvolemic patient points unmistakably toward solute deficiency rather than hormone excess.
Diagnostic Approach and Management
Diagnosis rests on a foundation no laboratory can replace: a thorough dietary history. A structured 24-hour recall or a simple open conversation about what the patient has been eating is the single most valuable diagnostic tool. Volume status assessment confirms euvolemia, distinguishing this syndrome from the hypervolemic hyponatremia of heart failure, cirrhosis, and nephrotic syndrome. Medication review should identify diuretics, SSRIs, and antiepileptics as potential contributors. Endocrine causes must be excluded with thyroid function tests and morning cortisol.
Management is, at its heart, nutritional correction, but it must be approached carefully to avoid the primary iatrogenic hazard: osmotic demyelination syndrome (ODS). Serum sodium correction must not exceed 8 to 10 mEq/L in any 24-hour period. Sodium should be monitored every 4 to 6 hours initially. Fluid restriction is appropriate if intake is high. Definitive treatment is dietary rehabilitation: gradual increase in protein intake toward and beyond 0.8g/kg/day, rebuilding the urea pool and restoring urinary osmole generation, accompanied by adequate sodium intake and dietitian involvement. In recurrent or refractory cases, oral urea supplementation at 15 to 30g/day represents a physiologically rational emerging strategy, directly augmenting urinary osmole excretion. Evidence remains largely observational but the mechanistic rationale is sound.
Management that addresses only the biochemistry and ignores the upstream cause will fail. Depression must be screened and treated. Social isolation must be interrupted through community referrals, family involvement, and structured meal programs. Treating tea and toast syndrome as SIADH leads to fluid restriction without nutritional correction, an approach that partially addresses the free water load while guaranteeing recurrence.

Public Health Implications, Prevention, and Future Directions
At the population level, this syndrome sits within a deeply concerning picture of geriatric malnutrition. Nutritional deficiency in the elderly is an underappreciated epidemic, compounded by food insecurity, poverty, and healthcare systems that prioritize acute illness over nutritional surveillance. The Mini Nutritional Assessment (MNA), a validated and simple screening tool, should be integrated into routine geriatric evaluation. Tea and toast syndrome, when detected, should be understood as a sentinel event signaling broader nutritional vulnerability rather than simply a sodium problem to be corrected and discharged.
Prevention is achievable and low-cost: adequate dietary protein at a minimum of 0.8g/kg/day, appropriate salt intake, avoidance of excessive low-solute fluid intake, community meal support programs, caregiver education, and regular serum sodium monitoring in high-risk individuals. True prevalence data remains limited, with most estimates derived from small case series and retrospective analyses. Prospective epidemiological studies incorporating dietary osmole assessment in elderly hyponatremic populations are needed. Oral urea supplementation awaits formal evaluation in randomized controlled trials. Dietary osmole assessment needs formal integration into standard hyponatremia evaluation protocols, a step that would likely improve diagnostic yield substantially at negligible cost.
Conclusion
Tea and toast syndrome is not a rare diagnosis. It is a quiet, preventable, and entirely reversible cause of hyponatremia hiding in the dietary histories of elderly patients who are rarely asked what they eat. Its mechanism is elegant in its simplicity: not too much ADH, not failing kidneys, but an empty osmole tank that limits the kidney’s ability to excrete water no matter how hard it tries. Its clinical signature, low sodium, low BUN, low urine osmolality, normal FEUric acid, euvolemia, and a diet of tea and crackers, is entirely recognizable if it is sought.
More than a nephrology case study, this syndrome is a mirror held up to the lived realities of aging: isolation, grief, poverty, and the slow erosion of something as fundamental as eating a proper meal. Addressing it requires clinicians to look beyond the laboratory and the medication list, and into the life of the patient sitting across from them. In the end, the most important diagnostic tool in tea and toast syndrome is not urine osmolality or Uric acid. It is the question: what have you been eating?
References:
Adrogué HJ & Madias NE 2000 Hyponatremia review
Link: https://www.nejm.org/doi/full/10.1056/NEJM200005253422107
Upadhyay A et al 2006 Incidence and prevalence of hyponatremia
Link: https://pubmed.ncbi.nlm.nih.gov/16585476/
Renneboog B et al 2006 Mild chronic hyponatremia and falls
https://pubmed.ncbi.nlm.nih.gov/16431193/
Gankam Kengne F et al 2008 Hyponatremia and fractures
https://pubmed.ncbi.nlm.nih.gov/18322138/
Waikar SS et al 2009 Mortality and hyponatremia
https://pubmed.ncbi.nlm.nih.gov/19470679/
Rowe JW et al 1976 Renal function and aging
https://pubmed.ncbi.nlm.nih.gov/938829/
Miller M 2006 Hyponatremia in the elderly
https://pubmed.ncbi.nlm.nih.gov/16431194/
Thaler SM et al 1998 Low solute intake hyponatremia
Demanet JC et al 1971 Beer potomania
Decaux G et al 2010 Urea for hyponatremia