
I. Abstract
Something unusual is happening in gyms, wellness clinics, tech campuses, and Telegram channels around the world. People are injecting themselves with compounds they ordered online, reconstituted from lyophilized powder in their kitchens, and dosed according to advice from strangers on Reddit. These compounds are peptides: short chains of amino acids that the biohacking community has anointed as the frontier of human optimization. The scale of this phenomenon has grown from a fringe curiosity into a genuine public health concern. Regulatory agencies are scrambling. Clinicians are encountering adverse effects they were never trained to recognize. And at the center of it all sits a fundamental tension that defines the entire crisis: these molecules are scientifically fascinating, potentially useful, and almost entirely untested in the people now injecting them.

II. Cold War Origins and the Wolverine Mythology
The story begins not in a Silicon Valley biohacker house, but in a secret military laboratory in Leningrad in 1973.
The Soviet Union had a problem: its soldiers, including submariners, missile operators, and fighter pilots, were aging too fast. The stress, the isolation, and a significant amount of radiation were breaking men down at the height of the Cold War, and worn-out soldiers were a strategic liability. The USSR Ministry of Defense brought in a military physician, Vladimir Khavinson, gave him a classified lab, and told him to fix it. What Khavinson found was stranger than anyone had anticipated; peptides are short amino acid chains that function as molecular signals, delivered to cellular machinery to dictate what to build, when to build it, and when to stop. Some of those messages, he found, could instruct an aging cell to behave like a young one. He spent the next four decades pursuing that finding, publishing 775 scientific papers, filing 196 patents, and treating cosmonauts, Chernobyl survivors, and submariners. He died in 2024 at 77, largely unknown in the West, his research sealed behind the iron curtain that kept it from the scientists who might have replicated or challenged it.

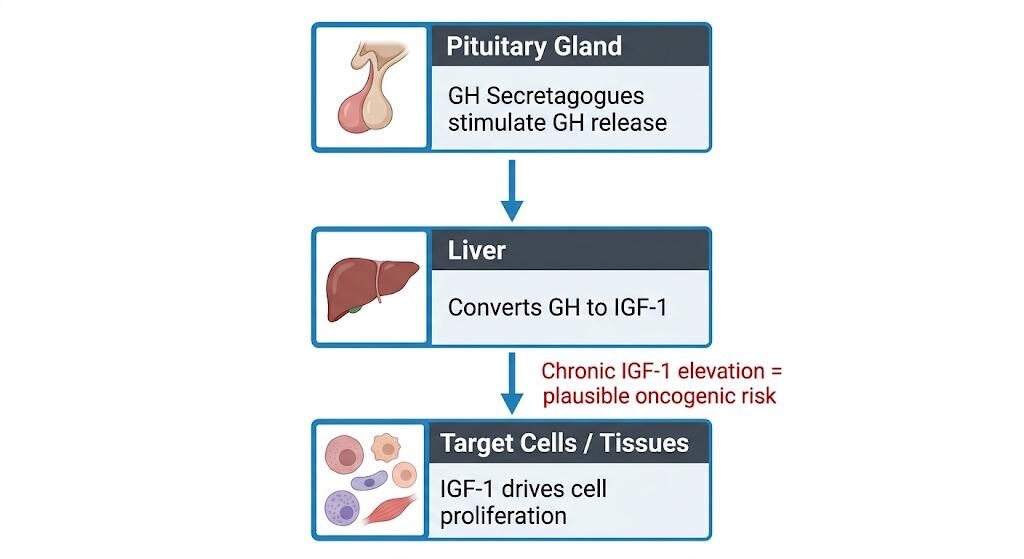
Simultaneously, the West was developing its own relationship with peptides, in a considerably sweatier setting. Through the 1980s and 1990s, bodybuilders had figured out that peptides could manipulate the pituitary gland into releasing more growth hormone. The peer-review process in this community consisted of one man in a gym telling another that it worked. For their purposes, that was enough.
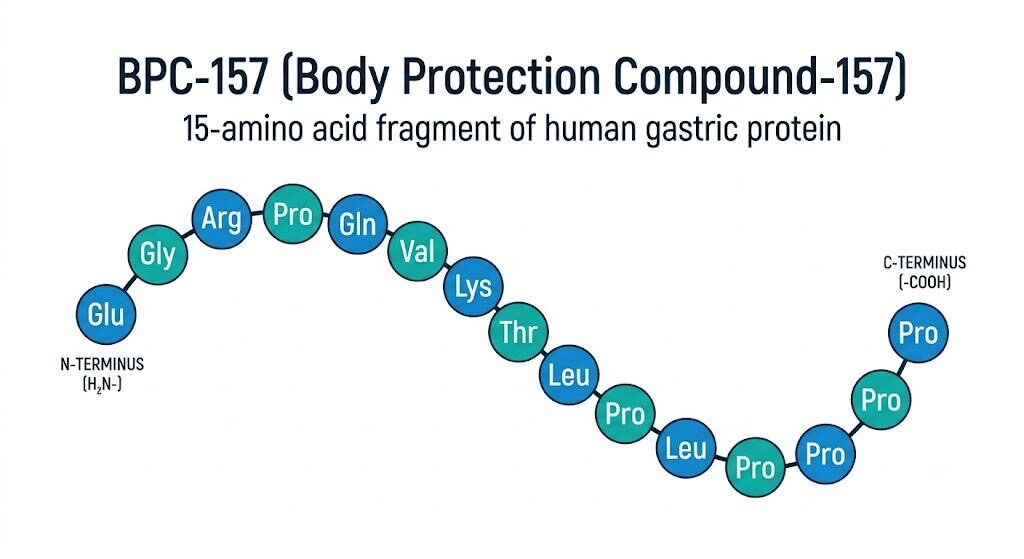
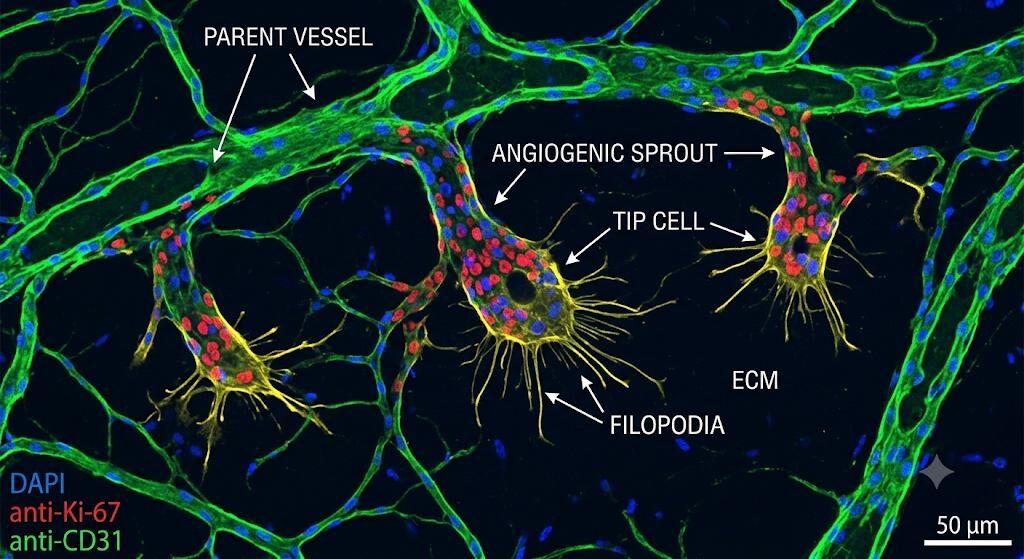
Then, in the early 1990s, a Croatian researcher at the University of Zagreb named Petar Sikirić did something that would eventually shake the biohacking world. He isolated a 15-amino-acid chain from a protein found in human gastric juice and tested it on rats. It healed things such as tendons, ligaments, gut tissue, and muscle fibre. This did not happen slowly or partially, but completely, at a speed that had no clinical parallel or framework to explain. The mechanism appeared to involve the aggressive stimulation of angiogenesis, which is the growth of new blood vessels, essentially rebuilding the entire blood supply to damaged tissue. He called it Body Protection Compound-157. The biohacking world named it after the only cultural reference that came close: Wolverine, the Marvel character who regenerates in real time. That name launched a billion-dollar underground industry.
III. The Subculture and Its Acceleration
To understand the peptide boom, you have to understand the culture that spawned it. Biohacking, which is the use of nutrition, technology, pharmacology, and self-experimentation to optimize biological performance, overlaps with longevity science, the quantified self movement, and bodybuilding culture. Its adherents tend to be male, educated, relatively affluent, and deeply skeptical of what they perceive as the medical establishment’s conservatism.
The communities where peptide culture lives are not hidden. Subreddits like r/Peptides have tens of thousands of subscribers exchanging dosing protocols and sourcing recommendations. Discord servers and Telegram groups operate in real time, with experienced users walking newcomers through the process of reconstituting lyophilized vials with bacteriostatic water and injecting subcutaneously. The advice is remarkably specific. The confidence is remarkable given the near-total absence of clinical evidence behind most of it.
On looksmaxing.com, an online forum where teenage boys obsess over optimizing their appearance through every available lever, including jawline exercises, posture correction, and skin routines, a thread titled “Would you guys recommend peptides for someone 17?” received this reply from a user with over 4,000 reputation points: “I am 16 on peptides and yes, I would.” The scale of this reached the attention of legislators; New York and New Jersey have both passed laws explicitly banning the sale of peptides and performance-enhancing compounds to minors, because teenagers were already buying them freely from vendors who asked zero questions.
Social media accelerated everything beyond what forums alone could have achieved. Podcasters with millions of listeners, including some of the most prominent names in the wellness space, discuss peptides in terms that blur the line between speculative excitement and factual endorsement. Gary Brecka, who styles himself the “Ultimate Human,” sells a $350 CJC-1295/Ipamorelin stack through his website. His marketing is a masterclass in sounding scientific while saying nothing: the “Who’s it for” tab on his product page targets “individuals incorporating peptide support into structured recovery, training or wellness protocols who want a synergistic dual peptide option that supports hormone signaling pathways and tissue maintenance.” Clear as mud, priced like crystal.
On July 4th, 2025, podcast host Jaden Clark was at a party in a San Francisco Victorian when an AI founder casually mentioned his Chinese peptide supplier. A crowd formed immediately. Everyone, it turned out, had a source. Clark posted about it on X: “Something I’ve learned is that the elites all have a Chinese peptide dealer.” The post went viral. The meme was accurate. Grey-market peptides have since flooded startup offices and hacker houses. One recent event at Frontier Town in San Francisco, which was a peptide rave sponsored by suppliers, featured a “mix your own peptides” workshop, a DJ playing techno while chemical structures projected on the walls, and a dress code calling for “crazy futuristic cyberpunk attire.” Attendees were shown how to draw their own blood. The FDA was not on the guest list.
At a Manhattan biohacker meetup, a tech investor described the scene: “Each week, someone will bring something new and everyone will inject it. It looks like a bunch of heroin addicts.” He said it as a joke. He has been microdosing peptides since 2018. One San Francisco supplier described the demographic diffusion pattern with accidental poetry; it always starts with the CEOs, then CTOs, then COOs. Biopharma people are shockingly the most reserved, being a little too deferential to the FDA. His average customer, he noted, is now closer to a Starbucks barista.
IV. Taxonomy of Commonly Abused Peptides
The range of peptides circulating in the grey market is now enormous, and each category carries its own profile of claims and hazards.
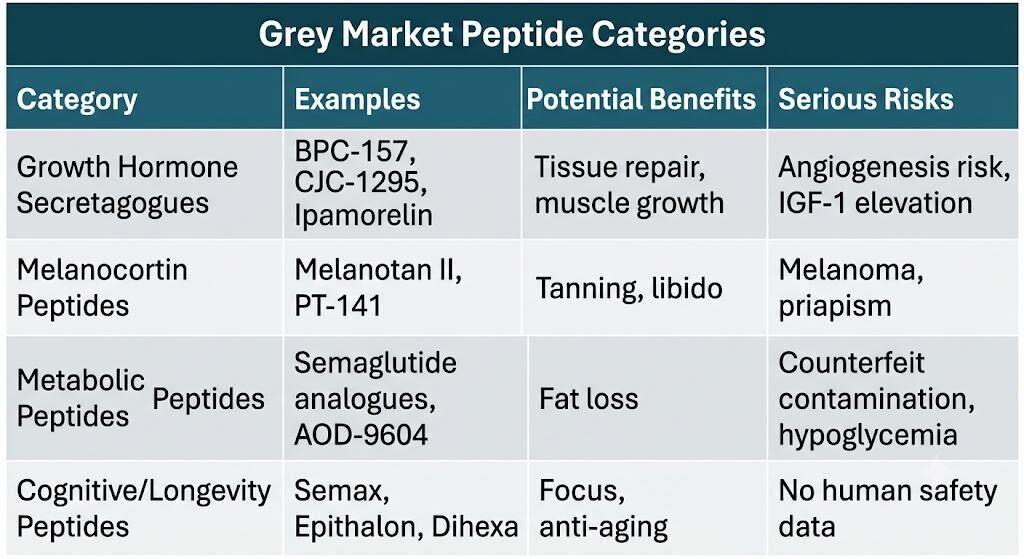
Growth hormone secretagogues form the most popular category. BPC-157, derived from human gastric protein, is marketed for gut healing, tendon repair, and injury recovery. TB-500, a synthetic fragment of thymosin beta-4, is promoted in athletic communities for tissue regeneration. CJC-1295 and Ipamorelin are frequently stacked for their synergistic amplification of growth hormone pulses, which users believe will improve body composition, sleep, and recovery. MK-677, technically not a peptide but an orally bioavailable growth hormone secretagogue, rounds out this category with the added attraction of avoiding injections entirely.
Melanocortin peptides occupy an entirely different category of concern. Melanotan II stimulates MC1R to deepen skin pigmentation through melanin production, and MC4R to modulate sexual arousal and appetite. It has become popular as a combined tanning agent and libido enhancer. PT-141, or bremelanotide, holds FDA approval for hypoactive sexual desire disorder in women but circulates widely in the grey market at uncontrolled doses for far broader uses.
Metabolic peptides now include the most alarming single development in the entire space: counterfeit and compounded analogues of semaglutide and tirzepatide. AOD-9604, a fragment of the growth hormone molecule, is sold specifically for fat loss despite an evidence base in humans that is essentially nonexistent.
Cognitive peptides include Semax and Selank, both of Russian pharmaceutical origin, claimed to possess anxiolytic and nootropic properties. Dihexa, developed at Washington State University for its synaptic potentiation effects, has attracted particular interest in the tech community, which perhaps explains why the line between Silicon Valley productivity culture and peptide biohacking has become so porous. At biohacker gatherings, oxytocin is being microdosed for “social optimization” — an OpenAI researcher has publicly described it as “Ozempic for autism.” Silicon Valley engineers are injecting a compound specifically to improve eye contact.
Longevity peptides represent the most speculative end of the spectrum. Epithalon is promoted on the basis of preliminary data suggesting telomerase stimulation and telomere extension, though the jump from that observation to “Epithalon reverses aging” is an enormous one that the existing data simply does not support. Humanin and MOTS-c, mitochondrial-derived peptides with genuine research interest behind them, are similarly marketed with claims that far outrun their evidence.
V. The Science Against the Claims
If there is one thing that distinguishes the peptide boom from ordinary pharmaceutical misuse, it is the magnitude of the gap between what the scientific literature actually says and what the biohacking community believes it says.
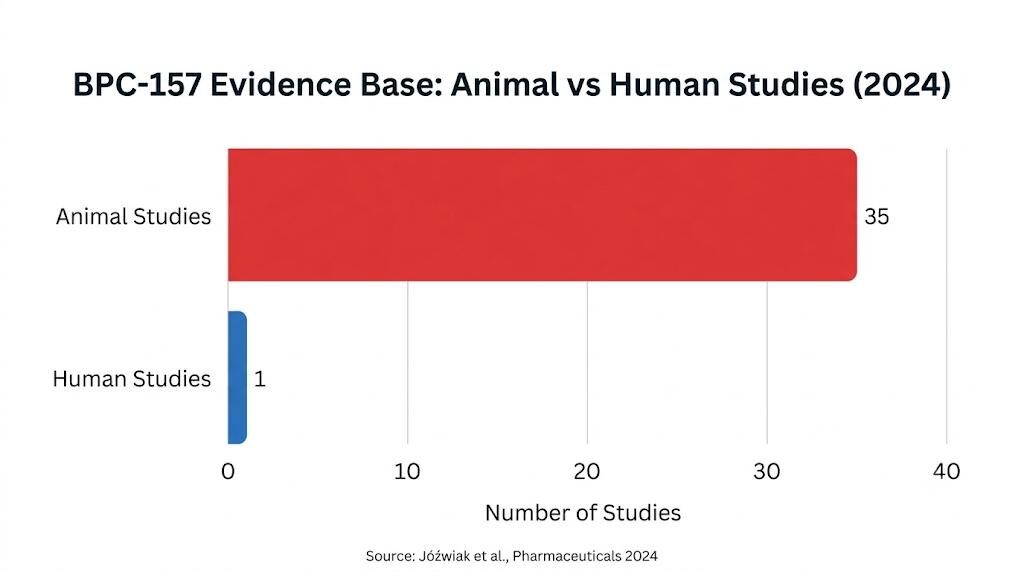
Take BPC-157. Its preclinical profile is genuinely remarkable: angiogenesis stimulation, tendon healing, and gastrointestinal protection in rodent models. Its advocates claim it has “the strongest evidence base of any biohacking peptide,” which is not entirely wrong within this specific universe. The problem is that “strongest evidence base” here means rats and cell cultures. As of 2025, the entire human evidence base for a compound injected by millions amounts to a retrospective study of 16 knee patients, a 12-patient bladder pain pilot with no control group, and a two-person intravenous pharmacokinetic study. Of 36 published studies on BPC-157 through 2024, 35 were conducted in animals. The vast majority of global BPC-157 research comes from a single laboratory, specifically the same lab in Zagreb where Sikirić first isolated it. A human clinical trial began in 2015. It was quietly cancelled in 2016. The results were never published. No explanation was ever given. Nobody followed up. Dr. Eric Topol, director of the Scripps Research Translational Institute, has called the entire peptide craze unfounded. Dr. Andrew Steele, upon reviewing the literature, was unequivocal: “I am shocked by how bad the evidence is.”
Epithalon’s situation is structurally identical. The telomere data driving its popularity comes from cell culture experiments and small animal studies. The inference from “telomerase activity increases in vitro” to “this peptide extends human lifespan” is not a scientific conclusion; it is wishful thinking wearing the costume of science.
Melanotan II presents perhaps the clearest case study in the consequences of misunderstood pharmacology. Its MC4R agonism, the mechanism users experience as enhanced libido, is the same mechanism responsible for spontaneous penile erections unrelated to sexual arousal. This is a side effect that appears repeatedly in the clinical literature and is reliably absent from forum discussions until it happens to a new user, who then reports it with considerable alarm. More seriously, multiple dermatology case reports have documented melanomas appearing in pre-existing naevi shortly after Melanotan II use, with Cancer Research UK explicitly stating that the drug is not safe in any form.
The angiogenesis concern deserves particular attention because it applies simultaneously to the mechanism that makes BPC-157 and TB-500 appealing and to the mechanism that makes oncologists lose sleep over them. Angiogenesis is how tumors grow. Cancer cells are not metabolically exotic; they require oxygen and nutrients delivered through blood vessels, just like every other tissue. One of the first things a developing tumor does is send chemical signals to recruit new vascular supply. This process is so fundamental to cancer progression that an entire generation of oncology drugs was developed for the sole purpose of blocking it. People are injecting compounds specifically designed to accelerate the formation of new blood vessels throughout their bodies. If those vessels are feeding a healing tendon, that is the intended outcome. If those compounds reach a cluster of subclinical precancerous cells, the result could be the pharmacological equivalent of pouring accelerant on a fire that was quietly burning at undetectable levels. No one has done the study, because the trials simply do not exist. However, it is a scientifically valid concern, raised repeatedly by researchers with nothing commercially at stake in either direction, and it is exactly the kind of signal that drowns in the noise of a forum full of people who currently feel fantastic.
Publication bias compounds everything. Positive animal results propagate enthusiastically through forums. Null results rarely enter community consciousness. And the grey literature that biohackers treat as scientific authority, such as vendor blogs, wellness clinic testimonials, and podcast conversations between non-researchers, is not remotely equivalent to peer-reviewed evidence.
VI. Pharmacological and Physiological Risks
The risk profile of peptide biohacking operates at several levels simultaneously.
At the most fundamental level, any injected compound carries the risks of injection itself: site reactions, subcutaneous infections, abscess formation, and in the context of non-sterile preparation, septicemia. Lyophilized peptide vials require reconstitution, and the process of drawing a measured dose from a vial that may have been stored incorrectly, shipped across international borders without cold chain maintenance, and manufactured in a facility with no pharmaceutical-grade quality control is not as straightforward as forum guides make it appear.
Immunogenicity is a more subtle but serious concern. Peptides can stimulate the formation of anti-drug antibodies, particularly with repeated administration. These antibodies can neutralize the peptide’s intended effect, but they can also, in some cases, cross-react with endogenous peptides the body produces naturally, leading to consequences that are difficult to predict and may take months to manifest.
At the system level, the endocrine consequences of chronic growth hormone secretagogue use deserve particular scrutiny. Sustained stimulation of growth hormone release elevates circulating IGF-1, and chronic IGF-1 elevation carries a plausible oncogenic risk independent of the angiogenesis concern. Cardiovascular risks from Melanotan II are documented in case reports: hypertension, coronary vasospasm, and priapism related to MC4R agonism have all been described. For Semax and Selank, the honest answer is that long-term neuroplasticity effects in humans are simply unknown, because the research has not been done.
The counterfeit GLP-1 situation has moved beyond theoretical risk into documented harm. Approximately 10 deaths and 100 hospitalizations in the United States have been linked to off-brand compounded semaglutide. Cases in Lebanon documented hypoglycemic episodes in 11 individuals who received suspected counterfeit Ozempic. The FDA has identified counterfeit products entering even the legitimate US drug supply chain, including vials with falsified lot numbers, non-sterile needles, and salt forms of semaglutide never evaluated for safety or efficacy. In one particularly alarming instance, compounded semaglutide was found to be contaminated with BPC-157, itself an FDA-prohibited substance, compounding one uncontrolled variable with another.
VII. The Supply Chain and the Quality Problem
The grey market quality problem is substantially worse than most users realize, and most users already know it is bad.
The journey of a typical grey-market peptide begins on the Chinese social media platform Xiaohongshu (Red Note), where suppliers operate with a confidence that suggests they have never once worried about consequences. One undercover journalist found a seller whose account displayed refrigerators packed with color-coded peptide vials; the moment contact was made, the conversation moved immediately to WhatsApp. There was a ten vials minimum order for $60 shipping, which is approximately $48 total for ten vials of tirzepatide, the active ingredient in Zepbound, which Eli Lilly sells to American patients for $399 per month. The markup between Chinese factories and US pharmacies is approximately 800%. Someone is making an extraordinary amount of money in that gap, and it is not the person doing the injecting.
US customs data records peptide and hormone compound imports from China roughly doubling to $328 million in the first three quarters of 2025, up from $164 million the preceding year. That figure almost certainly undercounts the true volume. Shipments arrive hidden in cosmetics packaging, labeled vaguely enough to pass inspection, or they are bulk-shipped to US addresses where individual domestic mailing labels are applied before final delivery. This is a reshipping operation that keeps the international leg of the journey invisible to inspectors. Customs and Border Protection has been aware of this system for years. Their enforcement record on personal-quantity peptide imports is essentially nonexistent.
The legal fiction holding the entire operation together is three words: “research use only.” Under US federal law, selling BPC-157 is technically permissible as long as it is marketed for laboratory research purposes. Every vendor website is accordingly wallpapered in disclaimers: “not for human use,” “for research purposes only,” and “not intended to diagnose, treat, cure, or prevent any disease.” It is a legal pinky swear, functioning as a liability shield that transfers 100% of the risk to the buyer. Both parties understand exactly what is happening. When a journalist asked a Chinese factory operator directly whether they knew their Western customers were injecting these products, the operator’s response was unambiguous: “Yes.” That was the entire answer.
Multiple independent studies have found that between 20 and 60% of grey-market peptides contain incorrect amino acid sequences. This means that nearly half of what people inject is not even the intended compound, but simply something else in a convincingly labelled vial. A significant proportion of tested samples have exceeded safety thresholds for endotoxin contamination, which refers to bacterial byproducts that, when injected, trigger systemic inflammation or, in serious cases, septic shock. Traces of heavy metals, such as lead, arsenic, and mercury, appear as residual synthesis byproducts in compounds being injected directly into the bloodstream. Two things can be simultaneously true: a vial may test as 99% chemically pure with the correct molecule and concentration, and still be a biological hazard by other parameters entirely.
The biohacking community’s response to this was characteristically resourceful. They crowdfunded money to send batches to independent testing laboratories, such as Janoshik in the Czech Republic and Finrich in Texas, that specialize in grey-market compound analysis. Results are posted publicly in forums and Discord servers. Vendors who pass get recommended; vendors who fail get publicly excoriated. It is a fully functioning consumer protection apparatus for an entirely unregulated market, built by amateurs on the internet in their spare time. The problem is that certificates of analysis are trivially easy to photoshop. Vendors can pass legitimate tests on one batch and quietly ship an entirely different one. Even a genuine, freshly issued certificate tells you nothing about sterility, nothing about endotoxin levels, and nothing about whether the compound was correctly stored. This is critical for peptides that degrade rapidly when exposed to heat or light, especially over a two-week journey from China in a cargo container.
VIII. The Regulatory Vacuum
The legal architecture governing peptides in most countries was not designed with decentralized biohacking in mind, and the grey market has exploited every gap in it.
In the United States, the FDA regulates drugs for human use, but vendors selling compounds labelled “for research purposes only” operate in a grey zone that makes straightforward enforcement difficult. The FDA has placed BPC-157, TB-500, CJC-1295, Ipamorelin, AOD-9604, Melanotan II, Selank, Semax, and several others on lists of substances not approved for compounding, on grounds of immunogenicity risks, peptide-related impurities, and insufficient human safety data. But this designation does not prevent vendors from selling the same compounds as research chemicals.
The 2023 FDA categorization decision that moved 19 popular peptides to the prohibited compounding list deserves particular scrutiny. The stated rationale was accurate as far as it went: insufficient safety data, immunogenicity concerns, manufacturing quality issues. But the move eliminated the one functioning middle ground in the regulatory landscape: licensed compounding pharmacies, where physicians could order peptides for specific patients under real quality controls, sterility testing, and genuine medical oversight. After 2023, demand did not decrease. It relocated — entirely and immediately — to WhatsApp suppliers in Guangdong province and to the veins of people who now had no legitimate alternative. The ban was intended to protect the public from unregulated injectables. Instead, it performed surgery to remove a splinter and accidentally hit an artery.
The situation was not, at its core, a straightforward market failure. Getting a drug approved costs anywhere from tens of millions to several billion dollars in clinical trials. The return on that investment requires a patent — twenty years of exclusive sales while every competitor watches from the sidelines. That is always the deal. The problem with peptides like BPC-157 is that they are fragments of proteins the human body already produces. You cannot patent something your own body makes. So nobody funds the trials. The FDA never gets the evidence it needs to approve them. The compounds remain in permanent legal purgatory: available to anyone with a credit card and a browser, impossible for any licensed physician to prescribe or licensed pharmacy to fill through standard channels. A law-abiding citizen has, perversely, fewer legitimate options than someone willing to buy from a stranger online.
In India, the CDSCO framework under the Drugs and Cosmetics Act covers Schedule H and H1 categories for prescription medicines, but most grey-market peptides are not classified under any schedule at all, creating an effective regulatory absence. The biohacking market in Indian urban centers, while smaller than its Western counterpart, is growing rapidly within the gym and fitness community. Australia’s Therapeutic Goods Administration has explicitly prohibited Melanotan II. The European Medicines Agency’s response remains inconsistent across member states. But even the strictest regulatory environments struggle against a supply chain that originates in Chinese synthesis facilities, transacts in cryptocurrency, and routes through multiple jurisdictions.
IX. Three Cases from the Field
The Trader Joe’s bag. A patient walked into a Washington DC physician’s office carrying a Trader Joe’s refrigerator bag. When she pulled out the syringes, her doctor assumed they were GLP-1s — Ozempic, Zepbound. They were not. The bag contained a “Wolverine stack”: a combination of peptides ordered online, promised to heal her torn rotator cuff faster than physical therapy. She had spent, in her physician’s words, “oodles of money” on a three-month supply and was injecting herself daily. “My trainer swears by it,” she said. “Everyone’s using them.” A stack, for the uninitiated, is exactly what it sounds like: multiple peptides layered simultaneously, each theoretically targeting a different biological system. Think of it as a custom medicinal playlist in which every track is an unregulated injectable, and hitting shuffle could give you sepsis.
Brooke Bowman. Brooke is 38, the CEO of Vibe Camp, an annual gathering of the rationalist community. She did everything the biohacking community considers responsible: she logged every injection in the Peptide Tracker app, monitored her sleep and resting heart rate obsessively, and obtained regular bloodwork. She began with BPC-157 and TB-500 for chronic fatigue, then added retatrutide — still in Phase 3 clinical trials — for theoretical cognitive benefits and to help her quit vaping. One day she accidentally doubled her dose. Her hair began falling out within a month. Her resting heart rate jumped ten beats per minute. She says she plans to keep going. She also mentioned, in passing, that she got clean from heroin in 2020. “Peptides scratch a similar itch,” she said. “I’m not getting that from heroin anymore, so it’s fun to have a new thing I’m experimenting with that isn’t horrible.” Another shipment from China was already on its way.
The RFK announcement. On February 27th, 2026, Robert F. Kennedy Jr. appeared on the Joe Rogan Experience and announced that 14 of the 19 peptides the FDA had banned in 2023 were about to be moved back from Category 2 to Category 1. Compounding pharmacies would be able to prepare them again under physician prescription within weeks. The biohacking community’s reaction was euphoric. Every forum and server that had spent years crowdfunding independent lab tests and trading Chinese supplier tips erupted. RFK himself called the original ban illegal and argued that it had created the very grey market it was supposedly designed to prevent. He is not wrong about the latter observation. The post-2023 grey market metastasized significantly. The number of people injecting unregulated, unsterile compounds from overseas increased, not decreased, after the prohibition on compounding. But the reversal, while genuinely meaningful in one narrow respect, does not resolve the deeper problem. There are still no clinical trials. There is still no safety data on what a decade of use looks like. The cancer question remains entirely unanswered.

X. Digital Platforms, Sport, and Clinical Implications
The role of YouTube, Instagram, TikTok, and podcasting in normalizing peptide use cannot be overstated. These platforms have constructed an environment where anecdote functions as evidence — where “my knee feels better after six weeks of BPC-157” carries the same epistemic weight as a randomized controlled trial in the minds of the audience. Joe Rogan, on record: “I had tendonitis in my elbow. I started using BPC-157 and it was gone in two weeks.” This is not an outlier. It is the information environment in which millions of people are forming health decisions.
In sport, WADA’s prohibited list includes peptide hormones and their releasing factors, and the detection of short-half-life growth hormone secretagogues remains technically challenging. BPC-157 is currently under USADA review, with the agency warning athletes explicitly that it could be added to the prohibited list at any time. Athletes using it for recovery are gambling simultaneously with their health and their competitive eligibility.
For clinicians, the practical implication is this: taking a biohacking history is now a clinical necessity. Patients presenting with unexplained IGF-1 elevation, dysplastic skin lesions, injection site infections, hormonal irregularities, or unusual cardiovascular symptoms should be asked directly about peptide use. Most will not volunteer the information — partly because they do not consider it clinically relevant, and partly because they anticipate judgment. Laboratory monitoring in known users should include IGF-1, fasting insulin, lipid profile, and careful dermatological surveillance. The mental health dimension also warrants clinical attention: a significant proportion of peptide use, particularly within the gym and bodybuilding community, is driven by body dysmorphic concerns rather than genuine health optimization goals, and Brooke Bowman’s case is a reminder that for some users, the compulsive self-experimentation is performing functions that addiction previously served.
XI. The Endgame
Several trajectories are converging.
The legitimate scientific pipeline is advancing. BPC-157’s pharmaceutical analogue PL 14736 is under development, and if it reaches randomized controlled trials with positive outcomes, it will substantially reframe this class of compound. The tragedy of the present moment is that widespread uncontrolled use of grey-market peptides is actively contaminating potential trial populations, making it harder to conduct clean clinical research on the very compounds that might deserve it.
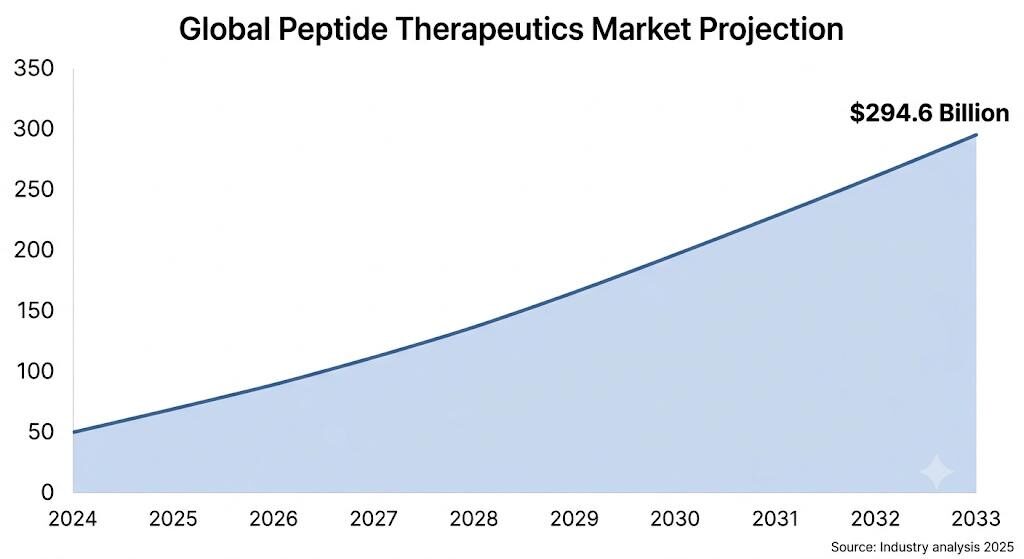
The pharmaceutical industry is positioning with the precision of a company that already knows the outcome. The legal global peptide therapeutics market is projected to reach $294.6 billion by 2033. Major pharmaceutical companies are closing acquisition deals worth hundreds of millions of dollars. The natural molecule cannot be patented and we have established that , but a modified analogue, a novel formulation, a new delivery mechanism can be. Tweak a few amino acids, file the claim, clear the FDA, and it is $400 per month for twenty years. The research use only loophole becomes legally untenable the moment an approved alternative exists. The grey market closes. The people who wanted these compounds are now channelled through a healthcare system those companies largely control. It is the oldest move in the pharmaceutical playbook and it has worked every time it has been run. The underground biohacking community spent years generating the real-world data that clinical trials are supposed to produce. The pharmaceutical industry will collect those results for free.
And then, most speculatively but most importantly, AI-assisted biohacking is emerging as a new frontier. Communities are beginning to use large language models to generate personalized dosing protocols and cycle recommendations for peptides, layering one poorly validated tool on top of another in ways that could produce genuinely novel harm patterns that existing pharmacovigilance systems are not designed to detect.
XII. Conclusion
The peptide boom is neither a simple story of reckless people doing stupid things, nor a story of medical gatekeeping blocking access to miracle drugs. It is something more uncomfortable: what happens when genuinely promising science encounters a culture optimized for hype, when regulatory frameworks built for pharmaceutical companies fail to anticipate decentralized self-experimentation, and when the financial interests of a grey market align perfectly with the psychological vulnerabilities of people who want to be stronger, younger, leaner, and sharper than they currently are.
The molecules themselves are not villains. Many of them are legitimately interesting to researchers. The problem is context: the near-total absence of human clinical data, contaminated supply chains, the absence of medical oversight, and an information ecosystem that systematically understates risk while overstating benefit. What this crisis demands is a convergence of responses: regulatory frameworks that specifically address research chemical loopholes, clinical training to recognize peptide-related presentations, platform accountability for health misinformation with identifiable commercial beneficiaries, and honest public communication that neither condescends nor conceals genuine uncertainty.
The deepest irony at the heart of the peptide boom is that the people injecting these compounds are often doing so in the name of taking science seriously, essentially acting on emerging knowledge before the mainstream catches up. But science, practiced honestly, begins with admitting what you do not know. And what we do not know about most of these peptides, in humans, at the doses being used, over the timescales being contemplated, remains almost everything.
The underground was the clinical trial all along. The question is who gets the data, and what they do with it.
References
- Jóźwiak M. et al. BPC-157 and angiogenesis: Regeneration or risk? Pharmaceuticals. 2024; PMC12446177.
- Lee E. et al. Retrospective study of BPC-157 knee injections. Altern Ther Health Med. 2021.
- Lee E. et al. Pilot study on intravesicular BPC-157 for interstitial cystitis. Altern Ther Health Med. 2024.
- Topol EJ. The Peptide Craze. Ground Truths (Substack). July 2025.
- USADA. BPC-157: Experimental Peptide Creates Risk for Athletes. September 2025.
- Steele A. Quoted in BBC Science Focus Magazine: Most anti-ageing peptides don’t work. But these might. April 2026.
- FDA. Concerns with Unapproved GLP-1 Drugs Used for Weight Loss. Updated February 2026.
- FDA. Counterfeit Ozempic Alerts. Multiple updates 2023–2025.
- Pharmacy Times. Off-Label Semaglutide Linked to Deaths, Hospitalizations. 2024.
- UVA Today. Q&A: Should you trust trending peptide injections? March 2026.
- WADA. Prohibited List: Peptide Hormones and Releasing Factors. 2024.
- Cancer Research UK. Melanotan safety warnings. Current guidance.
- NABP. Rogue Rx Activity Report: Injectable Weight-Loss Drugs. 2024.
- MMIT Network. Accessing Weight-Loss GLP-1s: The Role of Compounding Pharmacies. 2025.
- US Customs and Border Protection. Hormone and peptide compound import data. 2025